|
|
| Please note: All files marked with a copyright notice are subject to normal copyright restrictions. These files may, however, be downloaded for personal use. Electronically distributed texts may easily be corrupted, deliberately or by technical causes. When you base other works on such texts, double-check with a printed source if possible.
| |
| Consensus and Canaries |
| About Medical Science and its Loyalties |
| by Karl-Erik Tallmo |
| (på svenska) |
 The article is also available as PDF for better printing. The article is also available as PDF for better printing.(This article is a sequel to "A Life Redirected: The Story of an Illness".)
WHEN SOME PEOPLE LEARN that you are electrosensitive and still work at the computer, they often give you an incredulous, pitying look. As if there were no degrees in hell. Some pollen sufferers can handle certain species of pollen, while others make them almost sick to death. Similarly, not all kinds of electromagnetic fields are the same to all people who are oversensitive toward electricity. For instance, I am writing this text in front of a flat LCD display, which I can endure much better than monitors with cathode ray tubes.
If, on top of that, you tell people that you are also mercury poisoned from dental amalgams, you can see that they really would like to ask if you believe in UFOs as well.
It is sad, but not only lay people have this attitude. The scientific establishment - as represented by, for instance, many of the doctors and nurses one encounters as a sick person - has it too. I know some electronsensitive people who have been thrown out of clinics because they wished to wait for their turn in a less intensely luminous place than the waiting room with all its fluorescent light tubes. I have, to my own surprise, heard myself present my case to a doctor with a sort of apologetic attitude: "Well, I am not sure if you are one of those doctors who believe in this kind of ailment, but ..." As if medicine had become confessional, all of a sudden. Or: "I am one of those 'chronically complaining women with aches all over', only the male type ..." - as an attempt to possibly move their professional center of empathy by using a little self-directed irony.
”In the eighties they said that electrosensitive people were afraid of new technology - especially computers. However, after many highly motivated people, who loved their work at the computer, had taken ill and got oversensitive to electricity, this argument got more scarce. ”
You can often detect a certain skepticism within physical medicine towards psychodynamics and different kinds of psychotherapy. These doubts are usually easily swept away when confronted with hard to understand physical symptoms. The rescue for the doctor is often a diagnosis called "somatization disorder".
As mentioned in the first of these two articles, a physician early on diagnosed my problem as "panic attacks". And the social insurance office wanted to put me in psychotherapy. A woman friend of mine, who is chronically suffering from what is probably fibromyalgia, went to a clinic to get some remedy for an acute infection, legs more swollen than usual, extremely severe pain etc. Without even examining my friend's legs, this female doctor stated that my friend's legs were not swollen, although one could see this just by looking. The doctor also scolded her for having taken Citodon (a strong painkiller with paracetamol and codeine phosphate, like Codalgin Forte or Tylenol III), pills she had kept from earlier: "You should take those pills only when you are in serious pain!" When my friend finally started to cry in desperation for not being taken seriously, the doctor said: "Are you really sure this is physical? I think you ought to go see a psychiatrist instead!"
Doctors of this caliber have often read Jan-Otto Ottosson's textbooks in psychiatry. Ottosson said this in an interview 1996:
The amalgam illness started when idols came out in the mass media. "I've been this ill, but after the removal of my amalgam fillings I feel better." Then, if patients identify with their idol, things like amalgam illness might spread far and wide.
Fibromyalgia is a condition with tender points on the body. It is the result of longtime stress. Those afflicted are mostly immigrant women doing hard work in the industry. They gain from being sick-listed by getting the right not to work.[1]
Due to the increased prevalence during the last decades of chronic fatigue, muscle and joint pain, all sorts of food allergies, hypersensitivity toward electricity etc., many doctors are today in their confusion searching for extra-medical explanations. Dr. Tore Leonhardt, assistant professor of practical medicine, wrote a couple of articles in the Journal of the Swedish Medical Association (Läkartidningen), where he regards fibromyalgia and chronic fatigue syndrome as new names for old ailments, the kind he believes occurs at turns of centuries:
However, one might also apply wider cultural perspectives, and point at sentiments of uncertainty about the future, which seem to get stronger at turns of centuries. We are witnessing, not only the change from the industrial to the information age, but also a disintegration of authority in the religious and political areas and increasing apprehensions about environmental pollution. Such sentiments could probably be a hotbed for feelings of inadequacy in each individual, and they might be channeled into some sort of somatization.[2]
Others guess that these symptoms are some sort of manifestation of New Age mentality, or that some people have a strange kind of phobia for modernity. Lars Jacobsson, professor of psychiatry in Umea in Northern Sweden, wrote the following in an article:
What these diseases of modernity have in common is also that there are no clearly demonstrable causal factors, at least not those presented by patient organizations or certain scientists. Typical for all these conditions is a non-specific and very diversified symptomatology, which is something well-known to every practicing doctor and which is often a sign of a general weariness of life [my emphasis/KET] which manifests itself through a multitude of symptoms.[3]
This notion of a weariness of life is often heard. In the eighties they said that electrosensitive people were afraid of new technology - especially computers. However, after many highly motivated people, who loved their work at the computer (I remember one especially - a computer coordinator at the airline company SAS), had taken ill and got oversensitive to electricity, this argument got more scarce. Then another argument emerged, however, that those afflicted had loved their jobs too much and worked too hard. And I suppose one might suffer from long periods with too much work and especially the conflict of having too much responsibility coupled with too little influence. However, claiming that those who get these illnesses would in general be miserable beings hostile to modern technology is not correct. Personally I got sick during a period, which I would characterize as the most stimulating in my life, and I have always been very interested in technology, not the least new technology. But I have never been attracted to any New Age ideas.
One also often hears that "a non-specific and very diversified symptomatology" would indicate a non-physiological etiology. But it is well-known that, for instance, mercury poisoning gives rise to dozens of symptoms. Drugs registered in the Physicians' Desk Reference are often described as having dozens of side-effects - not seldom of a very non-specific kind indeed. When such reactions appear, it is hardly a question of "somatization".
A group of scientists have coined the term "modern health worries" (MHW), referring to mainly four components, environmental pollution, toxic interventions, tainted food and radiation. This group, Petrie et al., carried out a study in which they asked 526 students about their "worries", possible symptoms and perceptions of health. "MHW were significantly associated with somatic complaints and ratings of the importance of health to the individual. We also found individuals with high levels of MHW had a higher rate of food intolerance and chronic fatigue syndrome (CFS)," the scientists found, and this is their conclusion: "The results of these studies suggest concerns about modernity do cause changes in the way individuals interpret somatic information and may play a role in undermining perceptions of health."[4]
So, if you worry about our modern world and what risks its environment might bring about, this seems to give rise to food intolerance etc. A textbook example of statistically simplified associations: if one finds two variables with high incidence within the same group in the study population, lo and behold - we have a causal connection. But how can one tell that those variables are related, that others do not interfere (so-called confounders), and how can one tell which of the variables is the cause and which is the effect? In the above example, it would not be unreasonable to imagine that people who suddenly have become allergic to certain foods, easily might suspect, for example, new additives, and therefore they adopt a critical attitude towards modern food industry and the treatment of its products. It would seem more far-fetched if they get suspicious about food they might have eaten for years, and suddenly develop an intolerance.
Some are extremely cocksure. The American radio doctor Dean Edell said in an interview in March 2001 at the web site Healthcentral:
I'm fairly suspicious that chronic fatigue syndrome is really a psychosomatic illness. I'm sure that multiple-chemical sensitivity is a psychosomatic illness. I'm absolutely sure that breast implant disease is psychosomatic. I am close to sure now that Gulf War Syndrome and TMJ [temporomandibular joint syndrome] are also psychosomatic.[5]
In a way it is harder to reject the psychosomatic argument than the notion of somatization, which is a more blunt denial of soma in favor of psyche ("absence of somatic foundation", as Ottosson describes one of the foremost signs of somatization syndrome).[6] The psychosomatic view, on the other hand, at least seems to imply a rather sensible linking of our physical and mental sides, which most of the time are split apart in such an unnatural way. However, doctors like Edell seldom advocate a full view of the whole human being, but rather that "its all in their heads."
Anders Lundin, head physician at the Danderyd hospital in Sweden, wrote an article on somatization in the Journal of the Swedish medical association (Läkartidningen) in the spring of 2002:
The notion of somatization does not imply a disapproval of the validity of the biomedical model, which is superior in explaining and understanding machinery illnesses, such as fractures, pneumonia, cancer or anaemia. The notion of somatization is to be applied when biomedical factors are insufficient in explaining the suffering and impairment of an individual, when concurring psycho-social factors are underrated or neglected.[7]
Jan Lidbeck, head physician at the Helsingborg hospital, also in Sweden, wrote a responding article, claiming that Lundin's line of reasoning is turbid and breeds problems:
If we don't understand a symptom, it is contradictory to describe it using a term with the intrinsic meaning that we think we know what this symptom is caused by (a "somatized" inner conflict).[8]
Lundin's wish to acknowledge both biomedical and psycho-social factors might seem as a rather attractive attempt towards a more holistic view. The problem, however, is that this very seldom is rooted in clinical practice. Lidbeck also writes:
We use the notion of somatization within a traditional dualistic model, where psyche and soma are separated. Therefore, one cannot in an uncritical fashion assume that doctors in general now will start using the somatization concept in order to express a more varied bio-psycho-social view on disease. It is quite the opposite, and this is what causes problems.
I myself recently consulted a doctor specializing in infections, who from the viewpoint of this dualistic model without hesitation found the biomedical aspect irrelevant. I had informed her that earlier tests of my blood had shown an elevated activity of several subsets of lymphocytes as well as NK cells, during a couple of years. She said, the reason for this could be either a latent viral infection or stress. She chose, however, to regard my symptoms of pain, fatigue etc, as a "somatoform condition", caused by stress - despite an hour-long interview with me, where I clearly described how I for several years have not lived a stressful life. Furthermore, she disregarded my earlier history of exposure to toxins, as well as a recent thyroid test showing two kinds of autoimmune activity. "The notion of somatization is to be applied when biomedical factors are insufficient", wrote Anders Lundin. One wonders how many biomedical factors one must be able to put on display, in order to avoid the somatization diagnosis.
In December 2000 the Swedish magazine "Ny Teknik" ("New Technology") published a polemic article by Patrik Wahren, Licentiate of Technology, who claimed that electrosensitivity is nothing but a phobia; furthermore, it is easily cured:
For months the symptoms are slowly being aggravated - a psychological conditioning is in progress. The problems occur when the individual is experiencing an exposure to fields. It is common that the individual tries to withdraw from being near all kinds of electrical equipment.[9]
I am not sure what kind of experience with electrosensitive people Wahren might have in his technological licentiate world, but as I have described in the first of my two articles, my own hypersensitivity came unannounced, without "conditioning", and very often I experience discomfort and can't understand the reason at first - until I discover fluorescent lights or halogen lamps nearby. When it comes to attempts to "withdraw" from electrical equipment, I suppose Wahren is suggesting some sort of irrational fear behind this behavior, since he also writes:
There are similarities between this more severe form of electrosensitivity and the phobias. Today, the latter may be successfully treated with Anafranil or Klomipranil.
If asthma or nut allergy were unknown afflictions today, I suppose people who avoid places filled with tobacco smoke or bread with nuts would be regarded as phobic - or hysteric. Otherwise, I believe it is a most rational reaction to shun places that are harmful to you, even if official sanctions for such behavior should not have been issued. The European Union's reaction to BSE (the "mad cow disease") in 2000 - wouldn't that have appeared to be mass hysteria only two or three years earlier? More from Wahren:
Unfortunately, many of the afflicted will probably not appreciate the pleasant message that their disease is an easily treatable phobia. Through all of the irresponsible writings most of them will be firmly convinced that electric and magnetic fields are harmful - against all scientific findings within this disciplin.
The American radio doctor Edell is on to something similar as Wahren, when he says:
Take something like multiple chemical sensitivity. These people get outraged when you tell them it's all in their heads (and we've proven it over, and over, and over it's all in their heads) but they still don't want to believe it. They want to be sick. They almost enjoy being the center of attention. There's something that is psychological that feeds on this. [10]
In the interview mentioned earlier Jan-Otto Ottosson also points to this concept of psychological gain, when he advises physicians about common pitfalls:
Instead, Ottosson says in the interview, this is the way to proceed when one encounters "somatization syndrome":
Indeed, quite a devilish plot that is being spun here, when the physician preferably should involve the patient's family in the attempts to make the patient realize that he/she does not have the problems he/she believes, and to get the patient to stop this unconscious form of theater where he/she is acting out this "role of being sick", in order to obtain a certain "gain", and the patient must not nurture "unrealistic" hopes of getting so much better.
The message is pretty much the same in the fifth edition of Ottosson's textbook "Psykiatri" ("Psychiatry"). "Somatization syndrome is primarily developed in individuals lacking independence and showing histrionic traits," he writes.[11] (Histrions were actors or jesters in classical antiquity.) Here he advises the doctors to-be about how this redefining procedure is executed. The first step is that "the patient should get the feeling of being understood" and the doctor should "react on the patient's feelings through questions and empathetic comments". And then:
The second step is to mediate an essentially normal finding of an examination in a way that is acceptable to the patient. One can say, for instance: "You have a certain tenderness over the large intestine, but otherwise I have not found anything abnormal in your abdomen", and then acknowledge the existence of the ailment in an empathetic way: "You obviously have had a lot of problems in your stomach" and possibly tie this to some negative event in the patient's life: "People might have these ailments when they are upset and it struck me that you have been crying a lot and slept very badly ever since your mother died. [12]
Then the task is to get the patient to more specifically tie certain emotions to certain symptoms:
If possible the patient's symptoms should be tied to some difficult life event. A question about whether somebody in the patient's family or close surroundings has had similar symptoms, might make the patient realize that he has identified with this person och may thus understand his own symptoms through his knowledge about this other person.[13]
Did someone mention conditioning?
So, are there no people at all then, who are only "imagining" that they are electrosensitive or poisoned by amalgam mercury? Well, there are probably a few such examples. There are people who are absolutely convinced that they have cancer, without this being the case. However, this fact does not mean that there is no such thing as cancer. Suggesting, like Ottosson, Jacobsson, Wahren et consortes, that a whole group of patients are prey to their own delusions is deeply offensive.
Furthermore, taking the patient's resignation or desperation as a pretext for the validity of the somatization diagnosis is almost excessively arrogant - especially in the light of this talk about letting the patient "get the feeling of being understood". Ottosson warns against patients with an appealing attitude:
The ailments are described in a way that by its exaggerations - "horrible," "unbearable," "throbbing," "not a wink of sleep" - arouses suspicion and skepticism in the examiner.[14]
What Ottosson calls the "dramatic, appealing attitude" is, however, maybe not a very remarkable demeanor of a seriously ill person, who may have been waiting a long time in vain for both a diagnosis and some form of treatment, and who is now confiding in a professional who is supposed to be an expert on both diagnosis and treatment. A situation where a sick non-expert consults a healthy expert is unequal already by definition.
Another physician treading the same path as Ottosson is Sören Nielzén at the Psychiatric Center at the University Hospital in Lund, Sweden. In his article "On psychosomatic illness" he mentions chronic pain, electrosensitivity, oral galvanism, back pain, and chronic fatigue condition [sic], and says:
The patient presents a set of problems in symbolic form, rendered as a somatical-medical problem. If treatment shall be effective, the conceptions of this must be clarified and one must get the patients to modify their concepts and experiences of the disease. This may happen only if they are imparted with a conviction of relationships, which are yet not known to them, that is, they must make up their minds to reflect, receive information, and finally sense and experience the new context.[15]
Shouldn't there be a possibility also for doctors to open up their minds to "reflection" and "relationships, which are yet not known to them"? Workers using chain saws or pneumatic drills frequently complained about feelings of numbness, pain, chronic fatigue etc. - but were often met with skepticism, until the 70's or 80's, when vibration syndrome more and more became an acknowledged concept.[16] Women who had undergone mastectomy sometimes got complications consisting of chronic pain, which mostly was interpreted as a psychological disorder, until the 80's when one discovered that the surgical technique that had been used till then, could damage a certain nerve.[17] Now back to the writings of Sören Nielzén:
At the initial position one must start with "that it is really something physical" and give the patient's interpretation security. [...] Assuming that the patient is malingering or less intelligent is not just unprofessional and reprehensible, but actually stupid, since a final analysis can make any system of delusions understandable.
This is yet another example of how to use the old trick "taking people's concerns seriously". The pretending party in such a situation is actually the doctor, who gives the impression to be really listening and understanding. The notion that "a final analysis can make any system of delusions understandable" suggests that the doctor starts his examination presupposing that his patient is delusional. Then it just takes an appropriate analysis to prove this. Which brings to mind the words of psychologist Abraham Maslow: "[...] it is tempting, if the only tool you have is a hammer, to treat everything as if it were a nail".[18]
|
|
It is refreshing, however, to find that there really are doctors, even psychiatrists, who don't follow the herd. In this issue of The Art Bin there is an article by psychiatrist Per Dalén about somatization and how surprisingly vague the ground for this diagnosis often is: Diseases that are not found in today's book of somatic diagnoses will in other words have to be mental. At once the physician even "knows" what caused all the symptoms, which is more rarely the case in somatic medicine.[19] American child psychiatrist Alan Gurwitt wrote a short article in January 2002, published on the mailinglist Co-Cure, with the title "On the morbid fascination with psychiatric morbidity": Every so often there is an upsurge of debate about the place of psychological problems in regards to CFS, FM, and ME [chronic fatigue syndrome, fibromyalgia, and myalgic encephalitis/KET]. As a psychiatrist who has been seeing patients with these illnesses since 1986, as well as following the literature closely, I have often been embarrassed by and angry at many of my colleagues who fall in line with self-declared "experts" who see somatization everywhere. Ever since the mid-1980's there have been "researchers", with an uncanny knack at cornering research funds because of their already-formed biases that are in synch with the biases of the funding government organizations, who declare CFS, FM, ME to have a psychological basis or, more recently and insidiously, avoiding specificity about etiology, indicate that CBT [cognitive-behavioral therapy/KET] and graded exercise will do the therapeutic job, thus in part implying a major psychological causative factor.[20] Unfortunately, these theories of somatization are not the only problem an undiagnosed patient might encounter when seeing a doctor. As I said earlier, of course it is a great relief to get a name for one's ailments, but if this is delivered too easily, in a careless fashion, it might be regarded rather as a dismissal. I know of a case where a woman received the diagnosis fibromyalgia, after the doctor had only pressed a little on her knees and at the nape of her neck. "You have got fibromyalgia, and nobody knows what causes it, so there is nothing to do", the doctor said, obviously relieved at the thought of not having to intervene with any kind of treatment. "On the other hand," he said encouragingly, "you won't die from it." I have often thought of how many doctors infantilize their patients, how they treat them like less knowing children. How difficult it must be then for children suffering from chronic fatigue syndrome, fibromyalgia or amalgam poisoning! Because, as a matter of fact, children are afflicted too. The newspaper The Scotsman reported in February 2002 that there are estimates that 25,000 children suffer from fibromyalgia (or ME) in the UK.[21] According to an Australian study, there were 5.5 cases of chronic fatigue syndrome per 100,000 children up to the age of nine, and 47.9 cases per 100,000 in the ages 10-19.[22] A child with such ailments, and without really empathetic and perceptive parents, might of course easily be dismissed as being lazy or lacking manners. I really feel sorry for children when their parents don't believe their complaints. Instead the parents might drag them out of bed in the morning, and send them off to school, although they can hardly stand on their feet and maybe have intense pains. In cases where, on the other hand, sick children have empathetic parents who really listen, the whole family run the risk of being regarded by psychiatrists as collectively nurturing a myth of illness, in order to hide, for instance, severe "relational disorders".[23]
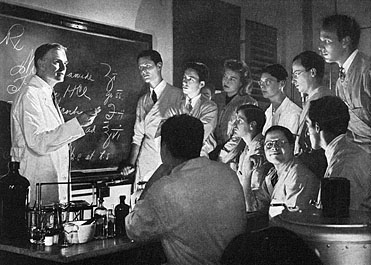
Let us now rise from the "clinic-floor", the level at which doctor meets patient, to the level of basic scientific research and politics, where the framework of health care practice is determined. Here we will find a couple of very frequently used rhetorical figures. One such recurring argument, which Patrik Wahren also used, is the notion that newspaper writings about the hazards of, for instance, living close to electric power lines or transformer stations, or using mobile phones, are irresponsible. At this level, among those using this rhetoric, it is also important to depict scientists who work with risk assessment regarding, for instance, mobile phones or dental amalgam as unserious cranks - especially if they actually assess a risk. Lars Jacobsson, professor of psychiatry, also says: It is not unusual that cited authorities are individuals in the margin of the scientific community, retired professors or even scientists who have been expelled since they don't meet the demands for scientific rigour that is required at universities and academies, or theoretical scientists in medicine with little or no contact with patients or knowledge of clinical practice.[24] Cancer researcher Lennart Hardell, professor of oncology at the University hospital in rebro, Sweden, who among other things have studied the hazards of dioxins and radiation from mobile phones, is one of several Swedish scientists who have been counteracted with the help of such arguments. Furthermore, he was one of those who warned that patients using certain antihypertensive drugs (so-called calcium blockers) run approximately a doubled risk of getting cancer compared to smokers.[25] The Swedish Medical Products Agency ignored the existence of the articles of Hardell et al. and claimed that no studies existed, that indicated any such risks with this type of drug. In 1997 a reporter at the Swedish investigative TV program "Norra Magasinet" asked Anders Ekbom at the Swedish Medical Products Agency about this, and he then admitted that "there is a rather explicit pecking order here regarding the quality of studies, and the rebro study just doesn't fit. Period."[26] During the spring and summer 2001 the same Ekbom, together with a few other scientists (Magnus Ingelman-Sundberg, Hans-Olov Adami, and Helen Håkansson), wrote polemic articles and appeared in radio shows claiming that unfinished research results are published carelessly in newspapers without previously having been peer-reviewed and published in the "correct" scientific journals. Again, professor Hardell was the main target, this time for his warnings that dioxins might be transferred to the baby through mother's milk. Without taking up a position on this particular issue, one might still note this interesting closing remark in the article: Publishing research, which does not allow for any certain conclusions, in forums with large penetrative power among the public, before the results have been reproduced by other scientists and attained scientific acceptance is something that creates considerable problems. This article [Hardell's article/KET] thus implies a contempt for those authorities, research financiers and scientists who work more long-term in order to reach reliable answers to these questions. It is unfortunate if such conduct injures the public's confidence in established, correct and important research results.[27] There was also an article - again in Swedish daily Dagens Nyheter - on September 23, 2001, where almost the same group of authors (Adami, Ekbom, Ingelman-Sundberg together with Lars Hagmar and Anders Ahlbom) persists in claiming that the public is not capable of judging from different views, in case the press would account for divergent research results. The authors have experienced that patients and the public express "confusion and resignation", and therefore "it is high time for both scientists and journalists to acknowledge their responsibility" by not publishing until consensus prevails.[28] As Lennart Hardell together with professor Gunilla Lindström say in response to the first article, such consensus might be long in coming, it might take centuries.[29] The prime example is probably the role of tobacco in inducing lung cancer. Most of us probably want to live in an open society with the freedom to form one's own opinion and avoid possible risk factors, even before they have been officially acknowledged and pertinent legislation has gained legal force. To hermetically confine research results within a close circle of peer-reviewers is hardly a prolific strategy. History is rich in examples of scientists who, owing to conservatism or prestige, have suppressed new ideas, coming from other scientists. Edward Jenner was ridiculed during twenty years for his ideas about cowpox contamination as a builder of immunity not just to cowpox - but to smallpox as well. A peer-reviewed journal rejected his research report in 1796, but Jenner published it privately in 1798. The Royal Society was still, however, reluctant, and did not want him to risk his (and the Society's) reputation by presenting "the learned body anything which appears so much at variance with established knowledge".[30] Lord Kelvin regarded Röntgen's discovery of X-rays as humbug. Liebig opposed Pasteur's ideas about the fermentation process as being a biological phenomenon and not a purely chemical one. When Mendel presented his conclusions about genetic inheritance based on statistical principles, there were many who held this to be some sort of number mysticism. In the case of Mendel, it took 35 years until consensus to some extent had been attained. The question is whether this would not have taken even longer if the matter had only been thrashed out internally, within the scientific societies in Brünn and Vienna. Waterston's contribution to the molecular theory of gases was stacked away for 45 years, because the article where it was described had been rejected by a reviewer in the Royal Society with the words "The paper is nothing but nonsense".[31]
There is an implicit dream that science will reach consensus regarding finally discovered truths. Knowledge increases through history as we ascend stairs of firmly established, finally proven conclusions and models regarding the world we live in. The French-American historian Jacques Barzun has written about this dream: "That hope may be the scientist's necessary illusion to keep him at work. We have read moving testimony that this is so; the historical fact is that scientific unity does not last long: the scientific generations change and disagree, and [...] not always by reasonable means."[32] (Image from a Parke, Davis & Co ad, 1941.)
Another striking example - within medicine - is of course Ignaz Filip Semmelweis, who in 1847 came up with the peculiar idea that the doctors after having performed autopsies, should wash their hands before they went to the maternity ward and examined the women there. When this routine had been introduced at the hospital in Vienna where Semmelweis was working, the rates of deaths from childbed fever decreased from 15-25 percent to around 3 percent. However, Semmelweis' colleagues did not believe there was a connection, so they stopped washing their hands, and the death rates increased again. For many thousand years we have built our knowledge upon trust. Nobody can on their own discover and experience everything. We simply have to believe that the earth is round and that viruses exist, even though we haven't been able to see this with our own eyes. Thus, knowledge of all kinds is a social contract, and new knowledge is successively admitted into it. In his book "A social history of truth", Steven Shapin writes about our modern dilemma: The village has given way to the anonymous city, relative simplicity of social structure to relative complexity. We trust the reliability of airplanes without knowing those who make, service - or fly them; we trust the veracity of diagnostic medical tests without knowing the people who carry them out; and we trust the truth of specialized and esoteric scientific knowledge without knowing the scientists who are the authors of its claims. Abstracted from systems of familiarity, trust is differently reposed but vastly extended.[33] If such a system of knowledge will hold through time and change without finally exploding like a too much inflated and expanded balloon, there is one requisite: public access. The demand for consensus before public access is absurd, not just concerning recently discovered risks. Demanding consensus is just as counterproductive concerning new possibilities, for instance, discoveries that could give us who are chronically ill the hope of finding a cure (here the Helsinki declaration from 1964 gives doctors the right, with the patient's consent, to try out new methods).[34] In the cases of chronic fatigue syndrome and fibromyalgia, there are a lot of causative theories flourishing, for instance, infections with CMV, Epstein-Barr, TWAR, rickettsia, herpes virus 6, or mycoplasma; protein leakage into the brain, malfunctioning activation of the enzyme calpain in the cell, too many blood platelets, too few blood platelets etc. - the half of it would be enough to get confused from contradictory ideas. But I prefer this, I prefer the possibility to study and learn and understand, rather than compact silence from the scientific community. The demand for consensus we hear today might seem alluring. The whole concept resembles our democratic tradition, where we vote and the majority decides. However, when it comes to scientific truth, factuality is the case, both when one person is right while a hundred are wrong, and when a hundred people are right while one person is wrong. The truth is the same. Scientists who trace risks must not be muzzled until their conservative colleagues might think fit to open up the floodgates for such reports. Today we know to what extent many scientists are dependent on financing from industry branches with a direct interest in a certain outcome of their research. Therefore, it is of no less importance to gain insight into the goings-on in the world of science than it is for the public to be able to monitor the world of politics and administration. Otherwise, much of what dwells with the scientists runs the risk of never even reaching the persons in this administrative layer - neither through direct contacts nor from those they represent, i.e. the people. When this information finally is disseminated in society, it might be just too undebated, biased and direct-delivered by lobbyists straight into newly awakened parliaments. This is the democratic aspect of the problem. In December 2001 Swedish daily Aftonbladet reported that epidemiologist Hans-Olov Adami works as a consultant for the chemical industry through the American PR firm Exponent, whose customers are, for instance, oil or chemical corporations.[35] In the fall 2001, soon after the debate Adami and his colleagues had initiated in Swedish media, he went to a conference in South Korea, "Dioxin 2001", where he in a lecture called in question that dioxin is carcinogenic. Together with, among others, Jack Mandel from Exponent, Adami also had written a report, "Dioxin and Cancer", which has been used in different versions by the American chlorine industry in order to convince the EPA that dioxin no longer shall be classified as carcinogenic. There are no ifs or buts in the conclusion of this report: "There is persuasive evidence that TCDD [dioxin/KET] at low levels is not carcinogenic to human beings and that it may not be carcinogenic even at high levels" [36] Consequently, it is hardly surprising that Adami has attacked Hardell, who 20 years ago was among the very first scientists that could show the connection between dioxin and cancer.[37] Adami is simply doing his job. "Adami gets paid to challenge his colleagues", as the reporter at Aftonbladet put it. In a sidebar he asks Adami:
Aren't you afraid that people will wonder if they can trust you and other scientists who act like this, when scientists are paid by those whose products they are supposed to examine? A debate about this broke out in the fall 2002, when the Swedish journals Medikament and Dagens Forskning (Today's Science) published articles describing the double loyalties of Hans-Olov Adami, on one hand as employee at the Karolinska Institute, with a professorship paid by the Swedish Cancer Society (the Society also provided Adami with a research grant, amounting to 6.4 million SEK), on the other hand the already mentioned consultancy assignments for the dioxin industry.[39] A representative from the Cancer Society was obviously shocked by this piece of news, in spite of the fact that Swedish evening paper Aftonbladet had published articles about this almost a year earlier. "This is a matter of utmost importance for the credibility of the Cancer Society", said Kenneth Nilsson, head of research at the Society to Dagens Forskning (no 18/2002).[40] And it should be. In 2001 the Cancer Society got 87 percent of its total income, a part amounting to 276 million Swedish crowns, from money collected from the public and donations drawn up in people's wills. Most likely, the donors are very interested to know that their money doesn't end up with people whose mission is to conceal cancer risks. The secretary-general of the Cancer Society, Marianne af Malmborg, promised to declare Adami's side assignments at the Society's homepage (www.cancerfonden.se). However, in the subsequent issue of Dagens Forskning (no 19/2002) the Cancer Society had changed its mind.[41] Now, Marianne af Malmborg says that "we don't have a police function" and "we have the greatest confidence in him [Adami] and in the Karolinska Institute". Apparently, some wheels in some machinery had moved during the two weeks between issue number 18 and 19 of Dagens Forskning. But which were they, and who turned them? Another Swedish scientist today, whom suspicion is cast upon, is associate professor Olle Johansson, who, for instance, has shown how electromagnetic fields affect mast cells in the skin, resulting in histamine emission and sometimes inflammation.[42] The Swedish Radiation Protection Agency is responsible for protecting the Swedish public from radiation hazards. Now, what is their position vis-à-vis Johansson's findings? In 1999 Kenneth Samuelsson wrote an article about this in Miljmagazinet (The Environmental Magazine): When I call Gösta Jonsson at the SRPA on the phone and ask questions referring to Olle Johansson's research regarding radiation and his knowledge, there is almost a defamatory attitude shining through in him. Gösta Jonsson says things like 'oh well, Olle Johansson plays his own game'. But when I ask him what he is insinuating, I get no further.[43] Klas Åmark, professor of modern history at Stockholm university, who has studied society's view upon work related injuries, says in the same article regarding how the SRPA has treated Olle Johansson: What is really awkward is that the authorities and those who want everything to go on as usual, try to get rid of scientists who are critical by attacking them or by trying to make them seem a bit odd and in that way marginalize them [...]. Ulrika Björkstén, formerly scientific journalist at Swedish daily Svenska Dagbladet, wrote this 21 May 2000:
Unfortunately a deadlock seems to have emerged, where those who engage in this field of research run the risk of being labeled as a bit nutty, or at least anti-progressive. It has all come down to a question of dangerous or not dangerous. And a large number of slipshod studies have given this field a bad reputation.
That microwave radiation has some kind of effect also on biological organisms is actually self-evident, at least at the atomic level. That microwaves are absorbed in our bodies means precisely that the electromagnetic field interacts with the matter that forms us. And just like the antenna of a telephone we ourselves are conductive. Therefore, the question shouldn't be if this affects us, but how.[44]
In March 2002 the news came that Director-General of the WHO, Gro Harlem Brundtland, is hypersensitive to electricity.[45] She gets headache from the radiation of mobile phones and asks everybody entering her office to switch off their phones. This was in the papers the same day as we were able to read other articles about WHO representative Michael Repacholi's attack on Lennart Hardell's research on radiation from mobile phones.[46] The future will show whether an afflicted person at such a high place possibly might lead to more unprejudiced judgments of research in this area at the World Health Organization.
Associate professor Mats Hanson (who also contributes to this issue of The Art Bin with an article about how the problems of dental amalgams have been known but neglected for 150 years[47]) is another scientist who is considered troublesome in certain circles. In 1985 he wrote an article in the Swedish midwife association's journal "Jordemodern" and warned about the effects of mercury upon the fetus: It is not recommendable to replace amalgam fillings directly before or during pregnancy, or during breast-feeding (mercury is transferred to the milk). When amalgam is drilled out one is exposed to vapor and amalgam dust in substantial quantities.[48] A dentist in Gothenburg then wrote to the Swedish National Board of Health and Welfare asking what advice to give to worried midwives. The board regarded this letter as a formally submitted complaint and wrote to Hanson's supervisor at the university of Lund: It is not the concern of the National Board of Health and Welfare to evaluate the scientific quality of publications issued at the university of Lund. However, according to the view of the board, the university of Lund should be anxious to assess the consequences of professor Hanson's publications. From the board's point of view, the following procedure would be preferable: With the help of the excellent international experts within mercury research as well as odontology, that the university have at their disposal, an evaluation should be made of the conclusions professor Hanson has drawn from the cited literature. The university of Lund will publish their viewpoints in the midwives' journal "Jordemodern". A prompt handling of the matter is necessary. [49] This letter was signed by Barbro Westerholm and Thomas Kallus. The rector at the university at that time, Hkan Westling, now dipped his pen and wrote back to the Board of Health and Welfare: The university as such does not evaluate the consequences of certain scientists' publications, nor will "the university" publish any viewpoints in some journal. Finally, it seems as if the Board of Health and Welfare wants the university to promptly issue some kind of report (of which the Board of Health and Welfare awaits a copy). What is probably implied by this statement are the viewpoints which were supposed to be published in the midwives' journal "Jordemodern". This is, as stated earlier, out of the question.[50] Mats Hanson also filed a complaint with the National Board of Health and Welfare, the Parliamentary Standing Committee on the Constitution, the Minister of Justice, and the Minister of Health Care. None of these, however, felt it necessary to consider any action in this matter, and in spite of the rector's unwavering attitude in his letter, Mats Hanson did not get his appointment as research scientist at the university prolonged. The irony of it all is that it did not take long before the National Board of Health and Welfare in their guidelines (statute code number SOSFS 1988:9) themselves advised pregnant women to as far as possible avoid going through any dental treatment with mercury amalgam. [51] This was almost retracted again in a statute 1991 (SOSFS 1991:6). It is difficult to follow all of the whimsical policy changes of the Swedish Board of Health and Welfare regarding dental amalgams, but the bottom line is that they have in fact been forced to withdraw from their original position more and more through the years. Strangely enough the very Barbro Westerholm who was the prime mover in the campaign against Mats Hanson later on presided in the special committee investigating ethics in science, which in 1998 published the book "Defending integrity in science and good practice in research".[52] Now, wasn't that letting the fox guard the henhouse! These are only a few examples of great talents in science, who in this manner have been subject to attempts of "marginalization", and then have been accused of being scientists of marginal merit. It is really sad, since it is a question of research that doesn't concern just a group of overstrung hypochondriacs or malingerers, as the critics of this research claim - in fact, it concerns the larger part of the population! Nearly all of us are exposed to, for instance, electromagnetic radiation or mercury emission from dental amalgams. We may avoid, for instance, meat or cigarettes if we wish to reduce the risk of getting Creutzfeld-Jacob's disease or lung cancer. But, when it comes to radiation or dental fillings it takes political decisions and a skilled dentist respectively, in order to avoid the risks. It is a matter of public health, political economy - and market forces. Of course, with the position Ericsson has in Swedish economy, it is in the short term inopportune to question the company's radiant main product. In the long term, however, research on the effects of radiation from mobile phones might turn out to be profitable and a means to acquire competitive advantage. Suppose that one day the hazards of this radiation will be proved, and the cherished consensus about this is attained, and the mobile phone manufacturers thus in a newly awakened fashion will have to start developing new safe products. Who will be in the better position then, if not those who awoke early and started working on a new safer technology? An parallel from business history is the Swedish ban on matches containing yellow phosphorus in 1901. Olav Axelson, professor of environmental medicine, says that this legislation most likely paved the way for the product development that eventually would produce the safety match, indeed a very lucrative business for Swedish industry. [53] Powerful economic interest groups fund research, obstruct research and even cover up research - we see examples of this almost every day. The already mentioned article by Lennart Hardell about side-effects from antihypertensive drugs was not cited by the Swedish Medical Products Agency, since they only read the references that the drug company submitted to them in its report.[54]
”The foremost example of how knowledge of side-effects from a drug have been cynically covered up is of course the case of thalidomide in the 60's.”
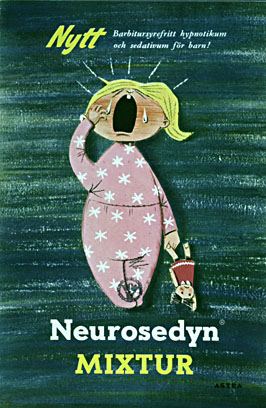
The foremost example of how knowledge of side-effects from a drug have been cynically covered up is of course the case of thalidomide in the 60's. The drug was manufactured on license and marketed in a number of countries (under a number of trademarks) as being the safest sedative ever produced. It had not even been possible to determine the lethal dose, Swedish pharmaceutical company Astra claimed in a brochure in 1960. Mice had been given 5,000 mg per kilogram body weight, which is an enormous amount, and on this level the testing was obviously abandoned.[55] However, lethality was not the problem. At the end of 1960 already, 1,600 reports concerning primarily neurological side-effects had been submitted to the main manufacturer Grünenthal in West Germany.[56] They took no notice of this, however, but tried to gloss it over and searched for scientists willing to vouch for the drug. Grünenthal also blamed some reported symptoms on the fact that users had combined the drug with alcohol - a peculiar argument, since the company had also marketed thalidomide as suitable for treatment of alcoholics.[57] The salesmen also tried their best to obscure the matter, for instance Dr. Goeden, who filed a report in February 1961 about a visit at a university clinic of neurology in Cologne: I declared our standpoint on the problem of polyneuritis and Contergan [the trademark used for thalidomide in West Germany/KET], and sought above all to cause confusion.[58] The company even claimed that thalidomide was especially suitable for pregnant women. In an ad in British medical journals they said: Distavel [the trademark used for thalidomide in the UK/KET] can be given with complete safety to pregnant women and nursing mothers without adverse effect on mother or child [...][59] Today we know that between 10,000 and 12,000 children were born worldwide, with malformed shortened arms, and sometimes also legs, a disorder called phocomelia. Grünenthal had, in fact, nothing that substantiated the claim that thalidomide would be safe for the growing fetus. And yet, in 1958 the company had sent the following message to 40,000 physicians: In pregnancy and during the lactation period, the female organism is under great strain. Sleeplessness, unrest and tension are constant complaints. The administration of a sedative and a hypnotic that will hurt neither mother nor child is often necessary. Blasiu has given Contergan and Contergan Forte to many patients in his gynaecological department and his obstetrical practice.[60] Swedish Astra also referred to Dr. Augustin Blasiu's article from May 2, 1958 in the journal Medizinische Klinik, and they claim that this article "reports good results from trials with gynaecological-obstetrical patients" [61] There was just one problem. In 1964, during the preliminary hearings preceding the West German trials, Blasiu said that he had never prescribed the drug to pregnant women, and in his article he had not written anything else than that he had given Contergan (thalidomide) to nursing mothers.[62] If one carefully reads the quotation from Grünenthal's 1958 letter above, one realizes the deceptive way in which it is phrased. It is not stated anywhere that Dr. Blasiu actually did give Contergan to pregnant women, and yet, this is the impression one gets.
Swedish brochure about Neurosedyn (the Swedish trademark for thalidomide) from the Astra pharmaceutical company (probably from 1961). The smaller print reads "barbituric acid free hypnoticum and sedative for children". In British ads, the manufacturer even claimed that thalidomide would be especially suitable for pregnant women.
Contergan was withdrawn from the West German market in November 1961, but still in 1966 Grünenthal tried to deceive public opinion by placing articles in German newspapers. On March 4, Christ und Welt published an article with the headline "What are the effects of Contergan? Scientific defenders of the sleeping pill" ("Welche Wirkungen hat Contergan? Wissenschaftliche Verteidiger der Schlaftablette"), while Hannoversche Allgemeine Zeitung on May 27 published the article "Experts criticize the Contergan theory" ("Experten kritisieren die Contergantheorie").[63] In a journal of sociology a certain professor Irle wrote that there was no evidence connecting Contergan with birth defects, and he also claimed that the investigations had not been impartial. All this happened during the preparations before the long drawn-out trials in Aachen and Alsdorf, which started at the end of the eventful month of May 1968. In spite of the fact that the rest of the world at last had woken up and banned the drug, changed legislation, and - as was the case in Britain - even adjudged damages to afflicted families, Grünenthal still managed to mobilize a number of unscrupulous scientists who claimed in court that there was no proof that thalidomide caused fetal damage.[64] Even a prominent person such as Nobel prize laureate Ernst Chain (one of the scientists who discovered penicillin) witnessed on behalf of the defendant. Let us go back again to 1960, when thalidomide was to be introduced in the United States. The licensed manufacturer here was the Merrell Company, and the trademark that would be used was Kevadon. Merrell struggled hard with the FDA to get the drug approved. Regarding the safety for the growing fetus, the company referred to Dr. Ray O. Nulsen from Ohio, a physician without special training in obstetrics. He was part of a group that clinically tested thalidomide, and he gave the drug to 81 pregnant women. Eventually, an article by Nulsen was published in the American Journal of Obstetrics and Gynecology, titled "Trial of Thalidomide in Insomnia Associated with the Third Trimester" (June 1961). The conclusion in the article was this: Thalidomide is a safe and effective sleep-inducing agent which seems to fulfil the requirements outlined in this paper for a satisfactory drug to be used late in pregnancy.[65] Some of the 81 women gave birth to children with phocomelia and during the trial hearings Nulsen revealed that his article had in fact been ghost-written by a Dr. Raymond Pogge from Merrell. The article was based on verbal reports that Nulsen had given to Pogge on the phone or at the golf course. There were no written records of the clinical trials which the article accounted for. There were quotations in the article from studies written in German, which Nulsen had not been able to read, since he did not master this language. In the thalidomide case the American FDA was very strict, thanks to Dr. Frances O. Kelsey, who insisted on evidence of the drug's safety. Owing to her efforts the drug was never introduced in the USA. Her tenacity contrasts immensely with the feeble passivity of the Swedish Medical Board (an earlier name for the National Board of Health and Welfare), which waited until March 1962 before it officially warned the public about thalidomide, even though the drug had been withdrawn from the Swedish market already in December 1961. For three whole months the Medical board thus allowed people who kept thalidomide in their medicine cupboards to continue taking it, unknowing of any hazards. In the Swedish press the board's representative later declared that they had not issued warnings since this "could have caused increased psychic stress in those mothers who were already pregnant at the time in question and might not have remembered the names of various drugs taken earlier in their pregnancy".[66] The FDA is otherwise not known as having a tough attitude toward the drug companies. Quite the contrary. Fraternizing with the industry had been going on for decades, and at the end of the 50's it was unveiled that the head of the antibiotics division, Henry Welch, had been receiving 287,000 dollars from the very antibiotics manufacturers over which he was supposed to exercise control. According to the book "Dark Remedy", the FDA officials socialized frequently with representatives of the drug companies. On Tuesday nights they used to dine at the Rive Gauche, an illustrious restaurant in Washington - and the companies paid the bills.[67] Regarding the Kevadon/thalidomide approval, Merrell had probably hoped that the FDA would not contact them to ask questions. At this time regulations stipulated that if the FDA did not act within 60 days after an application regarding approval of a new drug had been filed, the application would automatically be granted! Nobody had expected to encounter the competent Frances Kelsey, who was newly employed at the FDA and whose first assignment happened to be thalidomide. The FDA were, however, not persistent enough in 1982, when they gave the green light to an anti-inflammatory drug, Oraflex (benoxaprofen), despite the fact that there were 65 reports on side-effects, clearly related to the use of the drug. However, the drug company never mentioned these reports to the FDA. What they did report were instead 108 other side-effects which were not so clearly related to the drug.[68] Antihypertensive drugs were the topic at a conference organized by German company Bayer 1994 in Paris, with 500 invited physicians and medical journalists, who were to be persuaded of the qualities of a product called Adalat Oro. There was, however, one participant who asked troublesome questions about whether any long-term studies on lethality and myocardial infarcts had been made. This was Swedish journalist Ethel G. Ericsson, who was contacted after the meeting by an American scientist who wanted to tell her about a study that Bayer wished to keep secret. Bayer's representatives closely watched and disturbed the Swedish journalist and the American scientist in order to keep them from discussing the matter. Only on the dance floor did Ericsson and the scientist manage to get rid of their unwanted company, and then the Swedish journalist got to know that there really was a study that showed that the drug might induce a higher lethality caused by myocardial infarct.[69] When research results are to be brought out in practice at the clinics, doctors are, of course, key persons. That doctors who are there to give us who are ill the best possible care by making well-informed choices between available remedies and prescribe something that makes us better and not worse, is apparently not something one can count on. The marketing aimed at the doctors still seems to be as reckless today as in the 60's. Bayer's former press official in Portugal, Alfredo Pequito, claimed that he could prove that the company had bribed physicians all over the country. He has been the victim of two attempts on his life, the last one only a couple of days after he declared in the press that he had names of 2,500 Portuguese doctors who had received bribes consisting of travels and cash - their service in return was to prescribe Bayer drugs. Pequito was stabbed with a knife and had to be sewn up with 70 stitches, according to an article in The Guardian in September 2000.[70] Clinical work might be controlled in an improper way if physicians who work out guidelines for how a certain drug is to be used, have ties to the industry. In February 2002 the Journal of the American Medical Association (JAMA) published a study from Toronto, showing that nine out of ten doctors responsible for clinical guidelines for drug use in connection with cardiovascular disease, depression and diabetes, had strong ties to the drug industry.[71] Almost at the same time The Guardian reported that it is very common for scientists to put their bylines under articles they have not written themselves:
Ghostwriting has become widespread in such areas of medicine as cardiology and psychiatry, where drugs play a major role in treatment. Senior doctors, inevitably very busy, have become willing to "author" papers written for them by ghostwriters paid by drug companies.
Originally, ghostwriting was confined to medical journal supplements sponsored by the industry, but it can now be found in all the major journals in relevant fields. In some cases, it is alleged, the scientists named as authors will not have seen the raw data they are writing about - just tables compiled by company employees.[72]
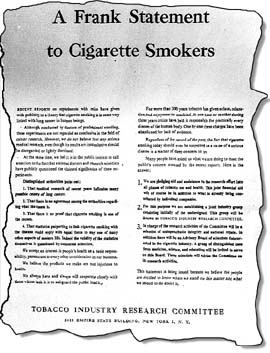
As if this wasn't enough, the spring of 2002 also brought the news that 3,500 German doctors were suspected of bribery. The company SmithKline Beecham (later renamed GlaxoSmithKline) had offered travels, events, computers, books and cash up to a value of 60,000 DM to German doctors. A company representative admits that these marketing methods have been used. [73] One can only guess what it looks like in the R & D departments of other criticized branches backed by powerful economic interests. Well, maybe guessing isn't necessary. Dr. Sheldon Krimsky at Tuft University, together with scientists at the University of California in Los Angeles, published a study in 2001 that scrutinized 61,134 scientific articles in 183 journals from 1997. Other studies had already shown that approx. half of all the academic researchers have done consultancy for the industry, and that approx. 8 percent have economic interests in the very branch their research pertains to. In spite of this, the study by Krimsky et al. now showed that only about half a percent of the articles declared personal interests or connections, such as consultancies, shares or patents.[74] In the summer 2001 the Swedish newspaper Ny Teknik reported that, for instance, the nuclear and forest industry fund professorships at the Royal Institute of Technology in Stockholm. There is no policy regulating how the independence of individual scientists shall be protected under such circumstances, and according to the article the rector Anders Flodstrm does not believe that this could be a problem. On the contrary, long-term agreements is a way of safeguarding this freedom, he claims: "We get to be more independent than in short-term projects."[75] Apparently, they were more worried about the freedom of science in Nottingham. Also in the summer 2001, British press reported that 16 members of a cancer research team at the university of Nottingham had resigned as a protest against the board's decision to accept a multimillion-pound grant from a tobacco company.[76] Already in 1996 the British Medical Journal reacted very strongly when Cambridge University were to accept a 1.5 million pound grant from the British American Tobacco Company (BAT). The journal claimed that this was as bad as if they would have accepted to launder money from the Colombian cocaine cartel. They also wrote that this kind of funding would open many potential conflicts of interest: If the academic who is appointed imagines that he or she is "independent" of such worldly considerations, the influence is, paradoxically, likely to be all the more insidious.[77] The tobacco industry's infiltration of research regarding the harmful effects of tobacco is, in fact, one of the most obvious and spotlighted areas where commercial interests have bought scientists, forged research results and tried to manipulate public opinion. After the big American tobacco trials at the end of the 1990's the tobacco industry was obliged to publish around 40 million document pages on the Web. This is a source that is hard to penetrate but very illuminating, since it clearly shows how big business will stop at nothing when it comes to tampering with truth in order to secure profits. By reading these documents, one gets glimpses of a brutishly systematic kind of disinformation one did not expect to find within the capitalist world, but rather in the Communist sphere. See, for instance, the Philip Morris Document Site, or the very useful meta search engine at Tobacco Documents Online.[78] The industry's counterattack picked up steam after the publication in 1952 of Richard Doll's and Bradford Hill's article in the British Medical Journal, where they on epidemiological grounds could ascertain that "the association between smoking and carcinoma of the lung is real".[79] At that time a few lab studies were made too, such as one made by Ernst Wynder et al., showing that 44 percent out of 81 mice developed tumors after having been painted with a tar concentrate made from tobacco smoke on their skin. [80] (This was, however, not the first experiment of its kind. Already in the 30's an Argentine scientist, Angel Roffo, had induced cancer in rabbits with a similar method. [81]) Now, the tobacco business responded by founding TIRC, the Tobacco Industry Research Committee, which advertised in 400 American newspapers in January 1954. The message to the public was that there is no evidence of any health risks, there is no consensus within the scientific community, people have enjoyed smoking for 300 years without problems etc. In June 1955 the chairman of the scientific advisory board of TIRC, Dr. Clarence Cook Little, was interviewed on television:
Question: Dr. Little, have any cancer-causing agents been identified in cigarettes? However, two years earlier the researcher C.A. Teague at RJ Reynolds Tobacco Co had compiled a confidential report on the current state of research, which of course was known to the TIRC. This is what is said under the heading "Conclusions": The increased incidence of cancer of the lung in man which has occurred during the last half century is probably due to new or increased contact with carcinogenic stimuli. The closely parallel increase in cigarette smoking has led to the suspicion that tobacco smoking is an important etiologic factor in the induction of primary cancer of the lung. Studies of clinical data tend to confirm the relationship between heavy and prolonged tobacco smoking and incidence of cancer of the lung. Extensive though inconclusive testing of tobacco substances on animals indicates the probable presence of carcinogenic agents in those substances.[83] Back to the interview with Clarence Cook Little 1955:
Question: Suppose the tremendous amount of research going on, including that of the Tobacco Industry Research Committee, were to reveal that there is a cancer-causing agent in cigarettes, what then? In a confidential report written in 1961, Philip Morris complacently stated that they had identified 50 new compounds, apart from 350 already known ones, that were constituents in tobacco smoke. [85] "Carcinogens are found in practically every class of compounds in smoke", they say and present a table of 48 carcinogenic compounds, (such as benzopyrene or benzanthracene), which is said to be just a "partial list". They also exemplify with 12 cancer promoting agents, such as phenols. But these findings were never made public, despite Little's promise.
In 1954 the newly founded Tobacco Industry Research Committee advertised in 400 American newspapers. Among other things the ad says: "For more than 300 years tobacco has given solace, relaxation, and enjoyment to mankind. At one time or another during those years critics have held it responsible for practically every disease of the human body. One by one these charges have been abandoned for lack of evidence." The text also says that many people have asked what the industry is doing to meet the public's concern aroused by the recent reports. The answer is the founding of this joint industry research group, the TIRC.
The TIRC sponsored scientists who wrote the "right" kind of articles. Up to 1961 there had been 197 such articles published by TIRC funded scientists, according to the head of research at the RJ Reynolds Tobacco Co, Alan Rodgman, who wrote about this in a confidential internal memo 1962.[86] The psychologist H.J. Eysenck admitted in his autobiography that he had accepted money from the tobacco industry.[87] In the British Medical Journal he published an article in 1960, presenting his ideas about lung cancer and that this disease was not due to smoking - but to personality.[88] In 1969 The New York Times refused to publish tobacco ads, unless they included a health warning together with figures showing nicotine content etc. This made the American Tobacco Company quite irate, and on September 4th they published a whole-page ad titled "Why we're dropping the New York Times", where they explained why they wouldn't buy ad space anymore: Sure there are statistics associating lung cancer and cigarettes. There are statistics associating lung cancer with divorce, and even with lack of sleep. But no scientist has produced clinical or biological proof that cigarettes cause the diseases they are accused of causing. After 15 years of trying, nobody has induced lung cancer in animals with cigarette smoke.[89] A number of lab studies had been done however, and within the business they discussed confidentially how difficult it would be to bring about some kind of safe tobacco "because known carcinogens are produced from such a wide variety of organic materials during the process of pyrolysis."[90] The discrepancy between what was said by industry representatives in public, and what was said internally, in confidence, was huge. Dr. Alan Rodgman, head of chemical research at RJ Reynolds Tobacco Co, wrote this in 1962: Obviously the amount of evidence accumulated to indict cigarette smoke as a health hazard is overwhelming. The evidence challenging such an indictment is scant.[91] In that paper Rodgman also commented on the matter which later The New York Times ad was about, that they did not wish to openly declare the constituents of tobaccco smoke on the cigarette packages: If a tobacco company plead "Not guilty" or "Not proven" to the charge that cigarette smoke (or one of its constituents) is an etiological factor in the causation of lung cancer or some other disease, can the company justifiably assume the position that publication of data pertaining to cigarette smoke composition or physiological properties should be withheld because such data might affect adversely the company's economic status when the company has already implied in its pleas that no such etiologic effect exists?[92] No animal studies proving a connection between smoking and lung cancer had been done, they said in the New York Times ad. But there were a few, and almost to the day five months after the ad had been published, the scientists Auerbach and Hammond organized a press conference (February 5th, 1970), where they presented a study on 62 dogs, of which 14 had developed lung cancer after having being forced to smoke.[93] The CEO of Philip Morris, Joseph Cullman, was interviewed on the CBC TV program "Face the nation" in January 1971, and he then rejected the dog study, claiming that most of the sick dogs had not been afflicted with lung cancer but with "invasive lung tumors" (tumors that spread to other locations than where they originated). Furthermore, the study had not been published in the "right" scientific journals, he said. It was at this occasion that Cullman delivered his notorious comment on a British study on 17,000 children born during the same week, which indicated that children with smoking mothers had a lower birth weight than children with non-smoking mothers. Cullman said that "it's true that babies born from women who smoke are smaller, but they are just as healthy as the babies born to women who don't smoke. Some women would prefer having smaller babies [...]"[94] During the following decades, the tobacco industry invested enormous amounts of money in the secret funding of scientists and their research. And services in return were certainly expected, because, as was said about one particular scientist, he "knows where his bread is buttered."[95] They made sure that books, articles and reports were printed, and ads aimed at the public were published, conferences were organized with the "right" participants etc. In 1970, Helmut Wakeham, head of research and development at Philip Morris, wrote the following to his CEO, Joseph Cullman: It has been stated that CTR [the Council for Tobacco Research, the successor of TIRC/KET] is a program to find out "the truth about smoking and health". What is truth to one is false to another. CTR and the Industry have publicly and frequently denied what others find as "truth". Let's face it. We are interested in evidence which we believe denies the allegation that cigaret [sic] smoking causes disease.[96] A quite remarkable attitude toward truth, considering that Wakeham is a person who says he is a trained Seventh Day Adventist. Wakeham is also a non-smoker.[97] The law firm Covington & Burling worked for the British American Tobacco Company (BAT) and drew up an elaborated plan for how the industry's so-called consultants (more or less secretly paid scientists) should work in the most efficient way in the USA, Europe, Australia, the Far East and Latin America. [98] In Britain they had managed to recruit a very prominent editor: Lancet. One of our consultants is an editor of this very influential British medical journal, and is continuing to publish numerous reviews, editorials and comments on ETS [environmental tobacco smoke/KET] and other issues.[99] At this time it was precisely this problem of passive smoking that had become a very hot topic for the industry. More and more public places were turned into non-smoking areas. Now, the industry tried to introduce alternate causes for lung cancer in non-smokers than tobacco smoke in their environment: The keeping of pet birds appears to be a major risk factor for lung cancer - a far more serious factor than anyone has ever alleged ETS to be. Two consultants have guided research on this issue conducted by others in Holland. A significant scientific paper was the result."[100] In 1998 Deborah Barnes and Lisa Bero at the University of California presented a study where they had investigated 106 scientific articles (from among other sources, the database Medline), containing reviews of studies of passive smoking from the years 1980-1995.[101] They found that 39 of the 106 articles concluded that passive smoking is not hazardous, and 29 of these 39 were written by researchers with ties to the tobacco industry. There are several Swedish scientists who on a regular basis have received payment for services to the tobacco industry. In December 2001 Swedish evening paper Aftonbladet reported that professor John Wahren at the Karolinska Institute, also a member of the Karolinska Institute Nobel Committee, had accepted more than 1.4 million SEK during the 1990's as remuneration for reporting about the doings of a colleague in the same corridor at the institute. This colleague worked with research on passive smoking, and of course Philip Morris was interested to receive "early warnings" if dramatic research results were on the way.[102]
”Toxicologist Torbjörn Malmfors became Philip Morris' coordinator for the expert group EGIL, a Nordic network of renowned scientists. Swedish members of EGIL were mobilized to fight the so-called Magnusson commission, which had the government's assignment to investigate tobacco advertising, taxation etc. ”
Other Swedes who were on the payroll at Philip Morris are Torbjörn Malmfors, assistant professor of toxicology, and Lars Werkö, a famous cardiologist. Malmfors became Philip Morris' coordinator for EGIL (Expert Group for Indoor Air), a Nordic network of renowned scientists. Similar groups were formed also in England (ARIA) and Asia (ARTIST). In the late 80's and early 90's, the greatest fear at Philip Morris was that the conclusions made by the American Surgeon General and the EPA, about the harmfulness of passive smoking, would spread to Europe. "Brussels is definitely 'lobbyable.' It is not often lobbied well, however", wrote the law firm Gold and Liebengood in a letter 1991 about the possibilities to manipulate European legislation.[103] In the attempts to influence politicians, it was also important to enlist members of two other professions. Contacts were made with scientists who could "reverse scientific and popular misconception that ETS is harmful".[104] And PM also directed their energy toward journalists, in order to "cast a shadow of doubt in media's mind".[105] The Nordic EGIL started in 1988 and consisted of seven Swedish, one Norwegian and eventually also two Finnish scientists.[106] As an example of the consultancy fees that were paid, it might be mentioned that Malmfors in January 1992 sent an invoice to PM's lawyers at Covington & Burling amounting to 19,725 dollars (120,320 SEK) for EGIL expenses during the month of December 1991. [107] One of the consultants that Malmfors recruited for EGIL was Lars Werkö, whom he knew since they both had worked at the research department at the Astra Pharmaceutical Company during the 1970's. Furthermore, Werkö had had contacts with the industry as early as in 1957, as a member of the Swedish Tobacco Company's special Medical Expertise Council.[108] In 2002 Werkö wrote a few articles in the Swedish press about the importance of science as independent of commercial interests. But they dealt primarily with, for instance, the drug industry and openly funded professorships at academic institutions. He did not mention secret extra-mural assignments - such as his own. During the debate that flared up during the summer 2002 in Sweden about tobacco money, Werkö said this to the Swedish daily Upsala Nya Tidning: "That passive smoking has immediate negative effects is quite clear."[109] Two years earlier - when there was hardly any debate at all about scientists with tobacco industry bias - he had said to another newspaper that "I was and am of the opinion that we don't know whether passive smoking is hazardous or not."[110] During the debate in the summer 2002 both Werkö and the medical insurance adviser, Dr. Bo Mikaelsson (who was also recruited to EGIL by Malmfors) claimed that their consultancies were only a matter of doing some literature studies, "peruse the scientific literature concerning ETS" (Werkö), "critically examine scientific articles" (Mikaelsson). [111] The aim of such activities is made clear in a Philip Morris document from November 1987, saying that the company wanted to support the Nordic consultants' "efforts to drive the thinking of their colleagues via articles and comments in the scientific literature and through presentations during symposia. Develop their ability to testify persuasively in government hearings and to generate positive stories in the popular press."[112] Swedish members of EGIL were mobilized to fight the so-called Magnusson commission, which had the government's assignment to investigate tobacco advertising, taxation etc.[113] Today, many of these consultants defend themselves by saying that working for a tobacco company was not a controversial matter at the end of the 1980's or the beginning of the 1990's. But this is not correct. Ingemo Bonnier at the local Philip Morris office in Sweden says in a letter from 1992 that EGIL has "not been able to fulfill expected media work as the climate has been too hostile which has demoralized the group to perform publicly".[114] "I asked Torbjörn [Malmfors] many times who stood behind EGIL, but the only answer I got was that it was an assigner interested in indoor air issues", Bo Mikaelsson says to Swedish daily Upsala Nya Tidning, June 13, 2002. [115] "Of course, I had some suspicion that the tobacco industry might be the assigner, but my guess was also that it could be the American health authority", he also says in the article. I just wonder why American health authorities would have to resort to covert operations. I also wonder why a renowned scientist like Mikaelsson would accept to work for somebody whose name he was not supposed to know. But Mikaelsson probably knew. In a monthly report from October 1988, Helmut Gaisch, president of science and technology at Philip Morris in Europe, says that he had met Mikaelsson together with two other principals of PM research in Europe, Helmut Reif and Peter Martin. Jean Besques from PM's EEMA region (Eastern Europe, Middle East & Asia) was also present at this meeting.[116] In another document from August 1990, Stig Carlsson at the PM office in Sweden is instructed to speak with the lawyer David Morse "about a possible additional signatory for Mikaelsson's Gun Palm article".[117] With more or less assistance from PM, Mikaelsson had apparently written an article about the Swedish social insurance case of Gun Palm, which attracted a lot of attention within the tobacco industry. According to the plaintiff, Gun Palm had acquired lung cancer and died, due to environmental tobacco smoke at work. Mikaelsson's article was supposed to show "why these benefits [the insurance money to Gun Palm's family/KET] should not have been awarded and why the system should be changed".[118] In December 1991 Mikaelsson received 82,172 Belgian francs and in February 1992 he got 75,774 Belgian francs from Philip Morris, by way of Covington & Burling, to be deposited in a bank account in Luxemburg. [119] The Swedish scientists Rune Cederlöf and Lars Friberg who created the famous twin registry, [120] which has been of great value for several epidemiological studies, offered their services to Philip Morris in the 60's already. In 1968 Cederlöf issued a statement before the US Senate during the debate about warning labels on cigarette packages.[121] There is one PM document that shows how an early draft of Cederlöf's statement was not approved: "...I do think Cederlöf is capable of a better statement", wrote one of the PM lawyers in a letter the 14th December 1967.[122] Obviously, Philip Morris were later more satisfied with the phrasing of the statement, and Cederlöf also delivered a statement before a House committee in 1969. After this appearance PM released a press message claiming that the twin study had shown that the association between smoking and angina pectoris might be merely statistical and not causal, and furthermore that genetic factors were at least as strongly associated with cough as exposure to tobacco smoke.[123] In 1969 Rune Cederlöf and Lars Friberg were invited by Philip Morris (who used the University of Melbourne as a front) to Australia to participate in a couple of symposia, arranged by PM. Through their connections the tobacco company also saw to it that Cederlöf and Friberg were enticed by the prospect of receiving honorary degrees at the University of Melbourne.[124] According to a document from 1975 Friberg received grants from the Council for Tobacco Research (CTR) amounting to 40,095 dollars for the years 1973/74 and 43,923 dollars during 1975/77. [125] The most important actor of them all is, however, Ragnar Rylander, professor emeritus of environmental medicine at the University of Gothenburg and also head of research at the IMSP (Institut de Médecine Sociale et Préventive) at the faculty of medicine of the Geneva university. Chung-Yol Lee and Stanton A. Glantz at the School of Medicine at the University of California in San Francisco have written a report about the tobacco industry's influence on research and legislation in Switzerland, and they claim: Rylander [...] is one of the most active tobacco industry's scientific consultants in Europe. The budget allocated to him by Philip Morris in 1992 was "USD 60,000/year unrestricted research grant and USD 90,000/year consultancy" and Rylander later served as a member of Philip Morris' IARC Task Force which was established to stop or counter a study that the International Agency for Research on Cancer was conducting in Europe on the link between secondhand smoke and lung cancer.[126]
Rylander's key role in the worldwide game pertaining to the hazards of tobacco smoking goes back 30 years. Already in 1974 Rylander - with financial aid from Philip Morris - organized a workshop about passive smoking which "aimed at putting the facts in proper perspective", as Helmut Wakeham put it in a letter to one of the company's lawyers Alex Holtzman in July 1973. Wakeham recommended that Philip Morris and the rest of the industry immediately should pay a grant of 30,000 dollars to the University of Geneva. [127] The next year Rylander allowed Philip Morris to use his name in an article they wrote for him: Attached is a draft of a meeting summary written for publication in Science in the section of that publication identified as "Meetings". The draft has been prepared by Nick Fina at the Philip Morris Research Center as a ghost writer and is intended to be published over the name of Ragnar Rylander [...][128] In a letter to the director of scientific affairs at Philip Morris, Richard Carchman, written June 23, 1997, Rylander says that he has avoided to fraternize openly with the tobacco company's management: I have never been involved with any Philip Morris executive in meetings or contacts with outside persons, to retain as far as possible the image as an independent scientist.[129] Another scientist, who like professor Rylander has worked for the industry for decades, is Dr. Gary Huber who researched on emphysema at Harvard University. Later on, he broke his ties with the industry and testified against it in several trials. Huber says that by supporting his research, the industry bought itself time: They had information in their internal documents and internal research labs that was 15 years ahead of the outside world and they let us and they let others, Federal Government, go forward and spend hundreds of millions of dollars, countless hours in research that didn't need to be done if they had opened their doors. And the tragedy of that is a lot of money and a lot of wasted research time and careers. But the real tragedy is all the lives that have been lost.[130] In June 2002 the WHO published an examination of all available research on tobacco and cancer made since 1986, covering 3,000 studies. The investigators found that the already known cancer risks were greater than hitherto presumed. Furthermore, they found definitive evidence that secondhand smoke causes cancer. Cancer forms that earlier had not been associated with smoking but now showing a clear connection, was cancer of the stomach, liver, cervix, uterus, kidney, nasal sinus, and finally myeloid leukaemia (a form of leukaemia affecting granulocytes, not lymphocytes).[131] It is strange to find that almost at the same time, the American department of Justice executed an investigation to see if the tobacco companies have changed their viewpoints after the big trials. The report on this investigation, made on request by rep. Henry Waxman, showed that four of five major tobacco companies still question whether smoking causes disease, that all five tobacco companies deny that environmental tobacco smoke causes disease in nonsmokers, and that four of five companies don't consider nicotine as addictive. [132] This strategy of denial, distortion and concealment has also through the years been the strategy of the PVC industry (see, for instance, the formerly confidential documents from the American vinyl chloride industry at the web site "Trade secrets"). Already in the late 50's it was known that the vinyl chloride monomer is harmful, but research results showing this were only discussed internally. The larger part of the industry, consisting of, for instance, Conoco, BF Goodrich, Dow Chemicals, Shell, Ethyl Corporation, and Union Carbide formed a cartel of silence, where they signed mutual agreements in order to keep reports about injuries and research results about risks secret. The industry lied deliberately to the American National Institute for Occupational Safety and Health (NIOSH). It was well-known, for instance, that vinyl chloride dissolved the bone in the fingers of people working with it: Gentlemen: There is no question but that skin lesions, absorption of bone of the terminal joints of the hands, and circulatory changes can occur in workers associated with the polymerization of PVC.[133] Publicly the strategy was to calm people. But in the privacy of their offices the industry's researchers read reports, such as a Romanian article about neurological symptoms and liver damage resulting from vinyl chloride exposure, or a report by Dr. M.J. Lefevre about 11 cases of acroosteolysis (dissolution of the bone in the finger tips) at the company Solvay Chemicals, or maybe a study by Rex H. Wilson et al. about 31 cases of acroosteolysis, presented in a JAMA article.[134] In an internal letter dated 24 October 1966, the research coordinator at Union Carbide's plant at South Charleston, R.N. Wheeler Jr, presented the following summary of a meeting with the Manufacturing Chemists Association Occupational Health Committee:
1. There is a definite health problem related to polyvinyl chloride manufacture. But the confidentiality classification was not revoked. Publicly one would hear the same old song: there is no scientific evidence ... no consensus ... nothing indicates any risk ... etc. In the proceedings of the so-called Vinyl Chloride Technical Panel Meeting 1980, a group within the Chemical Manufacturers Associations (CMA), we may read a comment from one of the participants made at the end of the sessions: [...] we may find out what we do not want to know with regards to brain cancer. If company has a brain cancer questionable incidence, which Union Carbide has, then should people be contacted. Union Carbide does not want any contact with families.[136]
”In the same way as the tobacco industry tried to emphasize other causes than smoking for lung cancer, the vinyl industry invested money in alternative explanatory models. ”
In the same way as the tobacco industry tried to emphasize other causes than smoking for lung cancer, the vinyl industry invested money in alternative explanatory models: "Should consider what else could cause brain cancer, besides vinyl chloride."[137] The CMA worked very determinedly with disinformation, and already in the 80's they organized fake grassroot groups (also called astroturf groups), that is, networks of "ordinary people" who at a given signal may flood the mailboxes of congressmen or newspapers with petitions and letters to the editor. [138] In a report to the board of CMA, W.C. Lowray put it like this in September 1980: When your grassroots systems are fully developed, we should be able to call for your help and give several thousand letters, telegrams and telephone calls to Members [of the Congress/KET] in a few days, each with a stamp of local relevance and personal understanding of the issue.[139] In 1984 there were 88 of the member companies who had created special posts as "grassroots manager" in order to organize such groups.[140] The obfuscating continued year after year, and in a message to the press 1999, the CMA (or rather its successor, the CMA was now re-named the American Chemistry Council) had the nerve to write about a new study that it "confirms what we've known for the past 25 years: VCM [the vinyl chloride monomer/KET] is a known human carcinogen and there is a strong association with angiosarcoma of the liver." On the other hand, the press message says, there is no longer any risks, since production methods have improved thanks to the industry's own research. According to the CMA/ACC all this proves that "through appropriate risk management and sound science-based research, industry can and does effectively manage the risks associated with VCM ." [141] However, as late as in 1995 - 36 years after the first PVC risk reports - PPG Industries and the Vista Chemical Company issued this statement in a promotional article before the joint enterprise of opening a factory at Lake Charles in Louisiana: Study after study has confirmed there is no evidence that vinyl affects human health - not for workers in the industry, not for people living near vinyl-related manufacturing facilities, not for those who use the hundreds of vinyl consumer and industrial products.[142] If one considers 36 years to be a long time, one might compare with how long the hazards of mercury from dental amalgams have been known but denied - this has been going on for 150 years: there is no scientific evidence ... no consensus ... nothing indicates any risk ...etc. As Dr. S.J. Green, head of research at the British American Tobacco (BAT), once wrote (under strictly confidential circumstances, of course): Scientific proof of course, is not, should not be and never has been the proper basis for legal and political action on social issues. A demand for scientific proof is always a formula for inaction and delay and usually the first reaction of the guilty. The proper basis for such decisions is, of course, quite simply that which is reasonable in the circumstances.[143] Or Fred Panzer, at the industry association the Tobacco Institute: [the industry's strategy] has always been a holding strategy, consisting of - creating doubt about the health charge without actually denying it [...][144] This is obviously a practical strategy both for the tobacco and the vinyl industry regarding the attitude towards hazards that might be related to their products. The fact is, this strategy is typical for several branches. The delaying and the demand for absolute proof from the opposite party - while at the same time often possessing such evidence but keeping it secret - is typical for branches dealing with, for instance, asbestos, radon, dioxin, PCB, dental amalgam, fluoride etc. [145] Certain stanzas echo through the decades, from various industrial branches, like fixed phrases, like ceremoniously recurring choruses in antique drama: there is no scientific evidence ... no consensus ... nothing indicates any risk ... the public is confused by unfounded health scares ... When one sees this pattern repeated through history, over and over again - is it so strange that one easily acquires a sort of preliminary skepticism towards new inventions, maybe not towards the usefulness and necessity of them, but in that respect that one would prefer that the burden of proof regarding their safety should lie with those who try to introduce the novelty in question, that they would need to get the harmlessness of their inventions proved at independent research institutions, not that those who are worried must prove the dangers? This is, I believe, especially important when it comes to environmental factors that large groups of the population are exposed to, risks that one cannot by one's own choice or actions be protected from - here, I think, the need for great caution is not only reasonable but self-evident. It is impossible to prove that something is not dangerous, is an objection certain people raise. "One can, for instance, not even prove that raspberry juice is not carcinogenic," wrote assistant professor Björn Cedervall, professor Magnus Ingelman-Sundberg et al. in a polemic article about the safety of mobile phones in Swedish daily Dagens Nyheter in July 2002. [146] This seems to be the perfect way to make the state of scientific research appear both reassuring and hopeless at the same time. Of course, it is impossible to prove that something is a hundred percent safe, judging from all imaginable risk aspects. However, it is possible to study specific suspected risks, not risks in general but risks limited to a certain kind of exposure under certain circumstances, for example, alteration in lung tissue after long-time exposure to other people's tobacco smoking, or how a certain aspect of the brain's physiology is affected after a certain period of daily use of mobile phones. When it comes to finding such areas needing research, case reports are important. One can hardly depend on that scientists themselves will come up with some far-fetched connection or that epidemiologists will discover an unexpected relationship just as a spin-off from some study. Such things do happen of course, which is fine, but regarding public health policies one cannot depend on serendipity. And regarding more unusual effects, case reports ar not just important but crucial. It would not be possible to compile a catalog of side-effects, such as the Physicians' Desk Reference without reports on concrete cases and patient reactions. The people in the drug industry realize this, even though they, as we have seen, not always take action after receiving such information. Still, at a symposium in 1967, organized by the drug company Ciba, the chairman showed fairly good insights by saying: It took seventy-five years to suspect that phenacetin caused renal disease, thirty years that amidopyrine caused agranulocytosis and ten years that the tetracyclines disturbed bone development. This should be proof enough that the medical profession does not quickly discover what it does not look for.[147] It is often said that the fact that so many people have amalgam fillings in their mouths and don't get sick, or that so many people smoke without getting lung cancer, would prove that those who regard dental amalgam or tobacco smoking as serious health hazards are exaggerating. But all this is part of the strategy. Grünenthal used this argument regarding thalidomide in the 60's.[148] And a representative of the tobacco industry said this officially in 1967: The vast majority of smokers - even heavy smokers - never get the disease. One recent servey showed that 97.3 [barely legible numeral in the scanned document/KET] percent of white males who had smoked 18 years [barely legible numeral/KET] or longer were free of lung cancer.[149] On the other hand, we have this statement made in an internal document by Dr. S.J. Green at the British American Tobacco Company: Properties of systems such as temperature, entropy, information and indeed disease statistics tell us nothing about a particular identified individual within the system. [...] Thus the argument that since there are heavy smokers who do not die of lung cancer (and, of course the great majority do not) and because there are some rare cases of non-smokers developing lung cancer, this in some way proves that increased smoking in a population does not cause the increase in lung cancer deaths, is totally fallacious.[150] Swedish professor of history, Klas Åmark, wrote an article in the magazine Forskning och Framsteg ("Science and Progress") in 2000 about how difficult it is for medical science to handle the question of individual susceptibility. His starting point is the problem of electromagnetic fields and whether they induce illness or not: My guess is that electrosensitivity is one of many examples of cases where the connections contradict the scientific thinking of method. Normally one assumes that small doses of a harmful factor will cause small injuries in a few individuals, large doses will cause severe injuries in many individuals. Science will get serious problems if it will be evident that small doses may cause severe injuries in a few individuals. Such connections are hard to prove with normal scientific methods.[151]
”Could the current reports of headaches be the canary in the coal mine, warning of biologically significant effects? ”
In 1998 the biologist Allan Frey wrote an article about those who get headaches from using mobile phones: "Could the current reports of headaches be the canary in the coal mine, warning of biologically significant effects?"[152] Here, Frey refers to what is said about keeping canary birds in the mines of the 1800's. This gave an early warning, when the concentration of gases such as methane or carbon dioxide got too high, since the birds, who were more sensitive than the miners, dropped to the ground unconscious. Assistant professor Olle Johansson is also on to this idea in an interview made in 2001: Perhaps all healthy persons, i.e. in the sense not being electrosensitive, ought to be extra happy for the electrosensitive ones, since they have acted as a warning for all of us? It could be, that we will owe them a lot since they reacted in time to something which the main bulk of mankind did not.[153] So, is it possible then to take individual susceptibility into consideration when it comes to determining limit values for various harmful environmental factors? Regarding doses, authorities often establish values for the highest allowable concentrations of pollutants in food, water or air, or the amount of radiation we safely may let us be exposed to. There are, however, several problems with this method: 1) In many cases, there are no threshold values of this kind, over which there is injury, and below which there is no injury. Several toxins, that affect, for instance, reproduction, physiological development and growth, or substances that induce cancer, have effects at all levels except zero. And individual susceptibility can manifest itself at almost any level. 2) In our complex world it is impossible to estimate the effects of a certain environmental factor alone, since it will interact with other factors within the organism. What would the total effect be in an individual exposed to, for instance, dioxins, mercury, electromagnetic fields, tobacco smoke and car fumes? Could it be that more mercury is emitted from dental fillings if one sits in front of a highly radiating computer screen than otherwise? Could it be that workers in noisy environments get their ears damaged quicker if they at the same time are breathing air containing solvents? Already in 1978 Nobel laureate Arvid Carlsson wrote about the need to see the big picture, when he discussed the issue of general water fluoridation: In the future, our health authorities will be increasingly engaged in the problems caused by this burden [the chemical burden on our environment/KET], problems of very high complexity, considering the difficulty of getting a quantitative overview, the interaction between different elements etc. In our society we will need to invest more and more resources in order to keep chemical exposure down on an acceptable level. [154] 3 a) Sometimes, established limit values are in fact borrowed from other contexts and therefore misleading. In the debate on dental amalgams, authorities often try to calm us by pointing out that mercury exposure from fillings are below a limit value set for industrial workers. However, being exposed to mercury vapor from the mouth 24 hours a day is not comparable to breathing mercury contaminated air during working hours only. Furthermore, as Mats Hanson says in his article in this issue of The Art Bin, limit values in the industry are often based on conditions in the chloralkali branch, where the presence of chlorine reduces the body's uptake of mercury. Regarding radiation from various models of mobile phones, they are more and more often labeled with so-called SAR values (specific absorption rate). But these values refer to the thermic effects of radiation, which is only one part of the problem, according to several researchers. As mentioned earlier, assistant professor Olle Johansson has shown how the mast cells of the skin are altered by radiation from TV and PC monitors, a much weaker radiation than what may cause thermic effects. Furthermore, in the fall 2002 the Italian scientist Fiorenzo Marinelli presented a study which showed that (non-ionizing) mobile phone radiation increases apoptosis (natural cell death) in leukaemia cells, during the first 24 hours of exposure, but after 48 hours this effect diminishes and instead three genes are activated, which stimulate the growth of these cancer cells.[155] b) Sometimes limit values are set almost arbitrarily. Economical or political factors might be decisive. In the fall 2001, the European Union discussed how to establish a limit value regarding dioxin content in fish, so that the fishing industry would not be jeopardized.[156] In 1966 Swedish authorities almost happened to establish a limit value for mercury content in food fish to 0.5 mg/kg wet weight, but in order to save the fishery in the Vnern lake, the limit was hastily changed to 1 mg/kg.[157] Now it is acknowledged that this limit was set too high. How many have been exposed to unnecessarily high rates of this toxin during almost 40 years? When reading about public health, scientific research, environmental hazards and illness one often gets the impression that cancer is the all-pervading problem. If an additive, a solvent or some kind of pollutant is shown not to be carcinogenic, then this seems to imply that there are no other risks connected with it either. Of course, cancer is one of our greatest scourges, and its incidence seems to increase - due to environmental factors, many claim - but there are (as mentioned in this article) also many other serious health problems connected with, for instance, poisoning (mercury from dental amalgam, for example) or radiation (from mobile phones, for example): which might induce immunological, neurological, maybe even genetical damages etc. Zoologist Theo Colborn and her co-authors wrote the book "Our stolen future" (1996), and they say: With cancer as the ultimate measure of our fears, it was widely assumed that setting levels based on cancer risk would protect humans as well as fish and wildlife from all other hazards as well. So over the past two decades, pesticide manufacturers and federal regulators looked mainly for cancer and obvious hazards such as lethal toxicity and gross birth defects in screening chemicals for safety. Cancer has also dominated the scientific research program exploring possible human health effects from chemical contaminants in the environment. This preoccupation with cancer has blinded us to evidence signaling other dangers.[158] There are debaters who willingly and aprioristically embrace all kinds of technological innovations, it may be genetically modified foods or the third generation of mobile phones. Even worse, with empirical evidence at hand, some of them still neglect or try to diminish risks and warnings that in real practice have been shown relevant, as has been the case with, for instance, the BSE problem. If you don't chime in with this, you are technophobic or anti-development. I can assure them, however, that being seriously and chronically ill gives you an entirely different perspective, than that of healthy editors writing editorials using "after us the deluge" as a motto. You simply don't need any more afflictions. It is enough being bedridden with cramps and spasms, unable to get out of bed half the time - one just doesn't wish to play with the risk that, for instance, aspartame would be shown to induce neurological effects which might cause even more cramps and spasms, or some totally new symptoms. I know that the risks regarding my example aspartame have not been assessed, but it is enough for me to know that there are strong suspicions and scientifically fairly plausible theories about the possible effects of this substance upon the signal transmission of the brain, in order to keep me from imposing yet another burden on the physiological functions in my body that are already much too strained. At a time when scientists independent of the aspartame industry, whom I may trust, have shown with reasonable demands for certitude that it is safe, I might eat or drink something that contains aspartame, but not sooner.
”Every dollar invested in precautionary measures would probably save several hundreds of dollars otherwise spent for health care, pensions, sanitation, rebuilding, reconstruction, litigation etc. ”
I think this ought to be a sensible attitude also toward risks that could afflict society as a whole, especially if one considers not only human lives but also what it costs society. Every dollar invested in precautionary measures would probably save several hundreds of dollars otherwise spent for health care, pensions, sanitation, rebuilding, reconstruction, litigation etc. once an expected problem has manifested itself clear enough to be recognized even by decision makers.
By way of conclusion I nevertheless wish to report three positive happenings during the last two years.
This kind of self-regulation is one first step. Vigilance is needed in more and more areas, not the least in the contradictory maelstrom of information conveyed by modern IT. Fake grassroots groups were a common phenomenon already decades ago. The PVC industry's networks of private persons have been mentioned, and the tobacco companies formed smoking clubs with "engaged citizens" advocating the right to smoke as the "freedom of personal choice" (seemingly an attractive idea, but in reality this liberty is unexecutable since the true nature of the options at hand is either denied or distorted). On the Internet today one must also be wary of infiltrators on mailing lists. Often PR people assigned by various companies are participating in the discussions, without revealing their mission. The American PR agency Bivings Group offers a service called "viral marketing". According to an article in The Guardian, this is what they said at their web site www.bivings.com (this text has now obviously been removed): [...] there are some campaigns where it would be undesirable or even disastrous to let the audience know that your organisation is directly involved ... it simply is not an intelligent PR move. In cases such as this, it is important to first 'listen' to what is being said online... Once you are plugged into this world, it is possible to make postings to these outlets that present your position as an uninvolved third party [...][165] Sometimes people say that source criticism is something that ought to be a school subject, when one considers the amount of both information and disinformation that flood over us in our modern world. That is an excellent idea. However, to be able to make such judgments one needs - at the very least - a basic knowledge of the most important subjects. In this respect, it is a serious problem that interest in the natural sciences among students is decreasing (at least in Swedish schools). Elementary knowledge in these matters is precisely the key one needs to be able to evaluate what has been published about research results within the sectors devoted to environment and health. The well-known writer and polymathic scientist Jacob Bronowski wrote: The world today is made, it is powered by science; and for any man to abdicate an interest in science is to walk with open eyes towards slavery.[166] In their book "Laboratory Life", Bruno Latour and Steve Woolgar depict scientific research as a sort of factory, where mail, phone calls, laboratory animals, chemicals and energy are brought in, then all this is processed, and finally scientific articles are brought out.[167] If one views science in this way, as a product like any other, it is of course hardly surprising that it can also be custom-made on request for a buyer. It is inevitable that scientific research has assigners, private or public, but it can have only one loyalty - truth. Someone might think that this is self-evident. Or that it sounds like a grandiloquent closing argument in an American movie trial. If one considers this more thoroughly, however, it must be clear that this is the only possibility. Loyalty to truth must mean that one is at any stage prepared to be disloyal to political and financial interests - if there is a conflict. Truth-seeking is not incompatible with a keen debate, where scientists who might be wrong also participate - rather, free debate is a prerequisite if the truth shall be fished out. In such a discussion there must be room for those who warn about new hazards as well as for those who believe warnings are completely uncalled for. New discoveries and inventions must be scrutinized and their possibilities discussed by both lay people and specialists. And, it would only be a benign side-effect if such discussions also would happen to reveal that certain participants have hidden agendas. Finally, I wish to return to the level of medical practice: during the years to come, I believe an increasing number of doctors will realize that they must learn to cooperate with increasingly informed patients. For a long time, we have been laughing at witch doctors in so-called primitive cultures, who claim they possess a mysterious and esoteric power that nobody else can understand and that is not to be questioned. But twenty years ahead, we may look at some of the more arrogant doctors of today in the same way. Competent and skilful physicians who care about their patients will, however, always be held in high regard, today as well as tomorrow.
Notes: 1. Hansson B.O., "Ont i munnen - av psykiska påfrestningar", Colgate Tandhälsa no 2, 1996.[Back] 2. Leonhardt T., "Fibromyalgi - nytt namn på gammal 'sjuka'", Läkartidningen [Journal of the Swedish Medical Association] no 21, 2000.[Back] 3. Jacobsson L., "Vi värjer oss från kunskap: Det finns inga klara orsaksfaktorer till el-allergi och amalgamsjuka", Västerbottens-Kuriren, 22 July 1997.[Back] 4. Petrie et al., "Thoroughly modern worries. The relationship of worries about modernity to reported symptoms, health and medical care utilization.", J Psychosom Res, 2001 July;51(1):395-401.[Back]
5. "Dr. Dean Edell - is fibromyalgia a pain messenger problem?",originally broadcast on 8 March, 2001. 6. Ottosson J.O., Psykiatri, 5 ed., 2000, p. 411. [Back] 7. Lundin A., "Somatisering - en utmaning för sjukvården", Läkartidningen, 11, 2002, vol. 99, p. 1239. [Back] 8. Lidbeck J., "Somatisering - uttryck för en förlegad sjukdomssyn", Läkartidningen, 13, 2002, vol. 99, p. 1505. [Back] 9. Wahren P., "Elöverkänslighet - lättbotad fobi", Ny Teknik, 6 December 2000. [Back] 10. "Dr. Dean Edell - is fibromyalgia a pain messenger problem?", broadcast on 8 March 2001. [Back] 11. Ottosson J.O., Psykiatri, 5 ed., Stockholm, 2000, p. 413-416. [Back] 12. Ottosson J.O., Psykiatri, 5 ed., Stockholm, 2000, p. 413-416. [Back] 13. Ottosson J.O., Psykiatri, 5 ed., Stockholm, 2000, p. 413-416. [Back] 14. Ottosson J.O., Psykiatri, 5 ed., Stockholm, 2000, p. 411. [Back] 15. Nielzén S., "Om psykosomatisk sjukdom", accessed 16 December 2002. [Back] 16. Already in 1911 an Italian physician had indicated a connection between known symptoms and pneumatic machines. Not until the 70's, however, was this recognized as an industrial injury which qualified for economic compensation. Especially the neurological injuries were acknowledged at a conference in Stockholm 1986. See Gemne G, Pyykko I, Taylor W, Pelmear PL., "The Stockholm workshop scale for the classification of cold-induced Raynaud's phenomenon in the hand-arm vibration syndrome", Scand J Work Environ Health 1987 aug;13(4):275-8 [Back] 17. Thernstrom, M., "Pain, the Disease", The New York Times Magazine, 16 December, 2001. [Back] 18. Maslow, A., The psychology of science: a reconnaissance, 1966, p. 15-16. [Back] 19. See Dalén P., "Somatic medicine abuses psychiatry - and neglects causal research", The Art Bin, 7 January 2003. [Back] 20. Gurwitt A., "On the morbid fascination with psychiatric morbidity", Chronic Fatigue Syndrome and Fibromyalgia Information Exchange, CO-CURE@LISTSERV.NODAK.EDU, 11 January, 2002. [Back] 21. See Foster K., "Seen but not heard", The Scotsman, 19 February 2002. [Back] 22. Se Lloyd A. et al., "Prevalence of chronic fatigue syndrome in an Australian population", Med J Aust. 1990;153: 522-528. [Back] 23. Se Garralda M.E., Rangel L., "Childhood chronic fatigue syndrome", Am J Psychiatry, 2001 Jul;158(7):1161. [Back] 24. Jacobsson L:, "Vi värjer oss från kunskap: Det finns inga klara orsaksfaktorer till el-allergi och amalgamsjuka", Västerbottens-Kuriren, 22 July 1997. [Back] 25. The original results were published in Hardell L., Axelson O., Fredrikson M., "Case-control study on colon cancer regarding previous diseases and drug intake", Int J Oncology 1996;8:439-44. Further commentary brought on by the following debate was published in Hardell L., Axelson O., Fredrikson M., "Antihypertensive drugs and risk of malignant diseases", Lancet, 1996 aug 24;348(9026):542. [Back] 26. "Norra Magasinet", Swedish Television, 10 March 1997. [Back] 27. Ingelman-Sundberg M., Ekbom A., Adami H.O., Håkansson H., "Publicera bara brett accepterade forskningsresultat" [Publish nothing but broadly accepted research results], Dagens Nyheter, 15 April 2001. [Back] 28. Adami H.O., Ekbom A., Ahlbom A., Hagmar L., Ingelman-Sundberg M., "Vetenskapliga sanningar - för vem?" ["Scientific truths - for whom?" an umbrella headline for this article and one by Finn Bengtsson], Dagens Nyheter, 23 September 2001. [Back] 29. Hardell L., Lindström G., "Skrämmande mörklägga cancerrisker" [Obscuring cancer hazards is appalling], Dagens Nyheter, 22 April 2001. [Back] 30. Gordon R., The alarming history of medicine, 1993, p. 49. See also Lehrer S., Explorers of the body, kap. 8, eller "Edward Jenner and the Discovery of Vaccination", University of South Carolina, accessed 16 December 2002.[Back] 31. Se Barber B., "Resistance by scientists to scientific discovery", Science, 134, 1961, p. 601. Lord Rayleigh was the one who finally found Waterston's paper after all those years and attended to its publication. In a preface he wrote: "the history of this paper suggests that highly speculative investigations, especially by an unknown author, are best brought before the world through some other channel than a scientific society, which naturally hesitates to admit into its printed record matter of uncertain value. Perhaps one can go further and say that a young author who believes himself capable of great things would usually do well to secure the favourable recognition of the scientific world by work whose scope is limited, and whose value is easily judged, before embarking on greater flights" (Quoted from Waterston J.J., The Collected Scientific Papers of John James Waterston, edited, with a biography, by J. S. Haldane, Edinburgh: Oliver and Boyd, 1928, p. 209-210. Haldane in turn quoted this from the original source, Rayleigh's introduction to Waterston's paper in Philosophical transactions of the Royal Society of London. Series A, Containing papers of a mathematical or physical character, vol. 183, 1892.). [Back] 32. Barzun J., Science: The Glorious Entertainment, 1964, p. 287. [Back] 33. Shapin S., A social history of truth: Civility and science in seventeenth-century England, 1994, p. 411. [Back] 34. The Helsinki declaration, revised in 2000, says: "In the treatment of a patient, where proven prophylactic, diagnostic and therapeutic methods do not exist or have been ineffective, the physician, with informed consent from the patient, must be free to use unproven or new prophylactic, diagnostic and therapeutic measures, if in the physician's judgement it offers hope of saving life, re-establishing health or alleviating suffering.", see The Helsinki Declaration, paragraph 32. [Back] 35. Söderberg, L., "Nobelprofessor hyrs av kemijätte", Aftonbladet, 17 December 2001. [Back] 36. Adami H.O., Cole P., Mandel J., Pastides H., Starr T.B., Trichopoulos D., Dioxin and cancer, report, 7 August, 2000. [Back] 37. Hardell L., Sandström A., "Case-control study: Soft tissue sarcomas and exposure to phenoxyacetic acids or chlorophenols", Br J Cancer 1979;39:711-717. [Back] 38. Söderberg, L., "Att få betalt för arbete ser jag inte som något kontroversiellt", Aftonbladet, 17 December 2001. [Back] 39. Walhjalt B., "Greenwashing - en introduktion", Medikament no 6, 2002, p. 72-80 (PDF). [Back] 40. Heldmark T., "KI-forskare kritiserar cancerlarm på uppdrag av kemisk industri", Dagens Forskning, no 18, 23-24 September 2002. [Back] 41. Heldmark T., "Cancerfonden kollar inte forskares vandel", Dagens Forskning, no 19, 7-8 October 2002. [Back] 42. Johansson O. et al., "Cutaneous mast cells are altered in normal healthy volunteers sitting in front of ordinary TVs/PCs: Results from open-field provocation experiments", Journal of Cutaneous Pathology, Vol. 28:10, 2001, p. 513. [Back] 43. Samuelsson K., "Kamp för sanningen kan bli arbetsskada", Miljömagazinet, 29 October 1999. [Back] 44. Björkstén U., "Kommentar mobiltelefoner: Spännande forskning väntar", Svenska Dagbladet, 21 May 2000. [Back] 45. Dalsegg A., "Får hodesmerter av mobilstråling", Dagbladet, 9 March 2002. [Back] 46. Snaprud P., "Svensk forskare får hård kritik av WHO", Dagens Nyheter, 9 March 2002. [Back] 47. Hanson M., "A hundred and fifty years of misuse of mercury and dental amalgam - still a lesson to learn", The Art Bin, 7 January 2003. [Back] 48. Hanson M., "Fosterskadande effekter av kvicksilver", Jordemodern 98 (1985), p. 74-75. [Back] 49. Åberg J., "Etik åt makten - kvicksilver åt folket!" (One proof-reading error corrected in collaboration with Mats Hanson). [Back] 50. Åberg J., "Etik åt makten - kvicksilver åt folket!".[Back] 51. Socialstyrelsens allmänna råd om utredning av patienter med symtom som antagits bero på kvicksilverexponering från amalgam samt om användning av amalgam, SOSFS 1988:9. [Back] 52. Att värna om vetenskapens integritet och en god forskningssed: Rapport om vetenskaplig oredlighet, Kommittén om forskningsetik, 1998. [Back] 53. Axelson, O., "Some historical notes and remarks on prevention in environmental and occupational health", Int. J. Occup. Env. Health, 10:339, 1997, p. 345. [Back] 54. According to Björn Beerman interviewed in the Swedish TV program "Norra Magasinet", Swedish Television, 10 March 1997. [Back] 55. "Neurosedyn: barbitursyrefritt sedativum och hypnotikum", Astrameddelande no 1 1960, p. 2. [Back] 56. Brynner R., Stephens T., Dark Remedy: The Impact of Thalidomide and its Revival as a Vital Medicine, 2001, p. 41. [Back] 57. Sjöström H., Nilsson R., Thalidomide and the power of the drug companies, 1972. p. 193. [Back] 58. Sjöström H., Nilsson R., Thalidomide and the power of the drug companies, 1972. p. 193. In the German edition of this book, the quotation reads thus: "Ich trug unseren Standpunkt zum Problem Contergan und Polyneuritis vor und suchte vor allem Verwirrung zu stiften." (Sjöström H., Nilsson R., Contergan oder die Macht der Arzneimittelkonzerne, 1975, p. 66.) [Back] 59.Sjöström H., Nilsson R., Thalidomide and the power of the drug companies, 1972, p. 195. [Back] 60. Sjöström H., Nilsson R., Thalidomide and the power of the drug companies, 1972, p. 194. In the German edition of this book, the last part of the quotation reads thus: "Blasiu hat vielen Patientinnen in seiner gynäkologischen Abteilung und in seiner geburtshilflichen Praxis Contergan und Contergan forte gegeben." (Sjöström H., Nilsson R., Contergan oder die Macht der Arzneimittelkonzerne, 1975, p. 173.) [Back] 61. "Neurosedyn: barbitursyrefritt sedativum och hypnotikum", Astrameddelande no 1 1960, p. 8. [Back] 62. Sjöström H., Nilsson R., Thalidomide and the power of the drug companies, 1972, p. 195. [Back] 63. Sjöström H., Nilsson R., Contergan oder die Macht der Arzneimittelkonzerne, 1975, p. 220. According to Sjöström/Nilsson there was especially one journalist, Alfred Püllmann, who helped Grünenthal in propagating their views. [Back] 64. Sjöström H., Nilsson R., Thalidomide and the power of the drug companies, 1972, p. 228. The book mentions professsor of anatomy, Erich Blechschmidt, professor of pathology Karl Ferdinand Kloos and professor of orthopaedics, Anton Hopf. [Back] 65. Sjöström H., Nilsson R., Thalidomide and the power of the drug companies, 1972, p. 125. [Back] 66. Sjöström H., Nilsson R., Thalidomide and the power of the drug companies, 1972, p. 199. [Back] 67. Brynner R., Stephens T., Dark Remedy: The Impact of Thalidomide and its Revival as a Vital Medicine, 2001, p. 42, p. 40. [Back] 68. Kohn A., False prophets: Fraud and error in science and medicine, Oxford, 1986, p. 179. [Back]
69. Ethel G Ericsson told this story in the TV program "Norra Magasinet", Swedish Television, 10 March 1997: 70. Gonçalves E., "Drugs scandal whistleblower stabbed again", The Guardian, 17 September 2000. This scandal is called Bayergate in Portugal. See also the newsletter KCB. [Back] 71. Stolberg S.G., "Study Says Clinical Guides Often Hide Ties of Doctors", The New York Times, 6 February 2002; Choudhry N.K. et al., "Relationships Between Authors of Clinical Practice Guidelines and the Pharmaceutical Industry", The Journal of the American Medical Association, 287, 6 February 2002. [Back] 72. Boseley S., "Scandal of scientists who take money for papers ghostwritten by drug companies", The Guardian, 7 February 2002. [Back] 73. Se Tuffs A., "German doctors face investigation in drugs scandal", British Medical Journal, 2002;324:693 (23 March) and Bowers S, "SmithKline hit by inquiry into bribes", The Guardian, 12 March 2002. [Back] 74. Stolberg S.G., "Scientists often mum about ties to industry", The New York Times, 25 April 2001. [Back] 75. Andersson S., Johansson I., "KTH säljer professurer", Ny Teknik, 20 June 2001. [Back] 76. "University cancer team quits over tobacco aid", The Times, 12 June 2001. [Back] 77. Carnall D., "Tobacco funding for academics", The British Medical Journal 1996;312:721-722 (23 March). [Back] 78. An overview of web sites with tobacco industry documents is available at Centers for Disease Control and Prevention. Other valuable resources are the Minnesota Tobacco Trial Exhibits and the Tobacco Control Archive. The book The cigarette papers by Glantz, Slade, Bero, Hanauer & Barnes, is available for online reading. [Back] 79. Doll R., Hill A.B., "A study of the aetiology of carcinoma of the lung", The British Medical Journal 1952;1:1271-86. [Back] 80. Wynder E.L., Graham E.A., Croninger A.B., "Experimental production of carcinoma with cigarette tar", Cancer Res, 1953:13:855-864. [Back] 81. Roffo, A.H., "Durch Tabak beim Kaninchen entwickeltes Carcinom", Zeitschrift f. Krebsforschung, 33:321-32, 1931. [Back] 82. Murrow, E. R. "Transcript of Edward R. Murrow's Second TV Show on 'Cigarettes and Lung Cancer'", 7 June 1955. Bates: 11311595-11311602. [Back] 83. Teague, C.A. "Survey of Cancer Research with Emphasis on Possible Carcinogens From Tobacco [Increased Incidence of Cancer of the Lung Is Due to Increased Contact with Carcinogenic Stimuli]", 2 February 1953, Bates: CTRMN043168-CTRMN043190. [Back] 84. Murrow, E. R. "Transcript of Edward R. Murrow's Second TV Show on 'Cigarettes and Lung Cancer'", 7 June 1955. Bates: 11311595-11311602. [Back] 85. Wakeham, H. "Tobacco and Health - R&D Approach". 15 Nov 1961 (est.), Bates: 2024947172/7196. [Back] 86. Rodgman A., "A critical and objective appraisal of the smoking and health problem", 1962, Minnesota Trial Exhibit 18,187 (PDF), p. 11. [Back] 87. Eysenck H.J., Rebel with a cause, London, 1990. [Back] 88. Eysenck, H.J., et al., "Smoking and personality", British Medical Journal, 1960, 1, p. 1456-1460. [Back] 89. "Why we're dropping the New York Times", The New York Times, 4 sept 1969, Minnesota Trial Exhibit 3380 (PDF). [Back] 90. F.J.C. Roe, M.C. Pike, "Smoking and Lung Cancer", Undated [1965 or 1966?], Minnesota Trial Exhibit 11041 (PDF). Pyrolysis is chemical change brought about by heat, for instance, decomposition. [Back] 91. Rodgman A., "A critical and objective appraisal of the smoking and health problem", 1962, Minnesota Trial Exhibit 18,187 (PDF), p. 7. [Back] 92. Rodgman A., "A critical and objective appraisal of the smoking and health problem", 1962, Minnesota Trial Exhibit 18,187 (PDF), p. 13. [Back] 93. Hammond E.C., Auerbach O., Garfinkle L. et al., "Effects of cigarette smoking on dogs", Arch. Environ. Health, 1970;21:740-68. [Back] 94. "Face the Nation", January 3, 1971, CBS Television Network Transcript, Minnesota Trial Exhibit 10492 (PDF). [Back] 95. Philip Morris wanted one of their funded scientists, Dr. Williamson, to direct analyses of the lead content in tobacco smoke: "Also by Williamson doing the analysis, it would give us both the availability of any data generated as well as controlling just what numbers were released - Dr. Williamson 'knows where his bread is buttered.'" (Confidential Inter-office memo at the Richmond office of Philip Morris from R.W. Jenkins to Dr. T.S. Osdene, February 25, 1976, Bates: 1000016677/6678.) [Back] 96. Memo from H. Wakeham to J.F. Cullman III, 8 December 1970, Bates: 2022200161/0163 (p. 1). [Back] 97. The following statement was, contrary to the confidential memo to Cullman, meant for the public: "Although I have never been a smoker, as a result of my religious training as a Seventh Day Adventist, I believe that smoking is a personal choice to be made by each individual. I, therefore, have never attempted to force my own views on anyone else, including my children, one of whom smokes occasionally. Far from experiencing any "crisis of conscience," I have always been proud of my work and accomplishments at Philip Morris." (Wakeham H.R., Letter to writer Richard Kluger [who i.a. wrote the book "Ashes to ashes" about the tobacco industry], 29 April 1993 , last page, Bates: 2047645709/5716.) [Back] 98. Report on the European Consultancy Programme, Covington & Burling, London, March 1, 1990, Bates: 2500048956/8969. [Back] 99. Report on the European Consultancy Programme, Covington & Burling, London, March 1, 1990, Bates: 2500048956/8969. [Back]
100. Report on the European Consultancy Programme, Covington & Burling, London, March 1, 1990, Bates: 2500048956/8969. 101. Barnes D.E, Bero L.A. , "Why review articles on the health effects of passive smoking reach different conclusions", The Journal of the American Medical Association 1998; 279: p. 1566-70. [Back] 102. Österman, H., "Han spionerade åt tobaksjätte", Aftonbladet, 7 December, 2001. See also the following Philip Morris documents, Bates: 2028376656 och Bates: 2028376955. [Back] 103. Gold Liebengood; Bushong D., "Philip Morris' EC Capability". 17 April 1991, Bates: 2045756540/6547. [Back] 104. "Proposal for the organisation of the whitecoat project", February 1988, Bates: 2501474262/4265. [Back] 105. Carlson S.G., "EEMA Corporate Affairs: Action recommended on EPA issue", report, 22 October 1991, Bates: 2501205612/5616. [Back] 106. Bonnier I., "Ets Media Relationsplan Nordic Area, 8th Revised Version", 19 October 1992, Bates: 2028398185-2028398194 (sid 9). [Back] 107. Malmfors Consulting, "Invoice". 14 Jan 1992. Bates: 2023856348-2023856349. [Back] 108. See Rådet för Medicinsk Tobaksforskning and Swedish Match, History. [Back] 109. Spross, Å., "Visste inte att industrin betalade", Upsala Nya Tidning, 13 June 2002. [Back] 110. Cantwell, O., "Detta är fullkomligt oetiskt", Aftonbladet, 24 August, 2000. [Back] 111. Spross, Å., "Visste inte att industrin betalade", Upsala Nya Tidning, 13 June 2002. [Back] 112. Se "Corporate Affairs Plan: Regional Overview", 25 November 1987, Bates: 2501254715/4723. [Back]
113. "In Sweden, PM is working to move the NMA to challenge the Magnusson commission to a public ETS debate, featuring EGIL scientists." ("Journalist Programme, Nordic Area", 2 August 1990, Bates: 2023590040/0043 [p. 2].) 114. Bonnier I., "ETS Media Relationsplan Nordic Area, 8th Revised Version", 19 October 1992, Bates: 2028398185-2028398194 (p. 9). [Back] 115. Spross, Å., "Visste inte att industrin betalade", Upsala Nya Tidning, 13 June 2002. [Back] 116. FTR, Fabriques De Tabac Reunies S.A.; Gaisch, H.W., "Monthly Report Highlights 881000". 31 okt 1988, Bates: 2028441095-2028441109. [Back] 117. Memo from Charles Lister to Stig Carlson, 5 August 1990, Bates: 2023590037/0039 item 9, Lister mentions David Morse, who was a PM consultant at the law firm Jones, Day, Reavis & Pogue (Surrey & Morse). In 1969, while he was the president of the International Labour Organization (I.L.O.), he went to Oslo to collect the Nobel peace prize on behalf of his organization. Among other things Morse helped PM in toning down the warning labels on cigarette packages in Iceland. See Bates: 2024946671/6673. [Back] 118. "EEMA Regional Annual Report Regarding PMI Corporate Affairs Action Plan", 16 October 1989, Bates: 2500019962/9976. [Back] 119. See Bates: 2023592948/2951 and Bates: 2023856353/6357, where the money is deposited in the name of "Saratoga Finance". [Back] 120. See Karolinska Institutet, "Världens största tvillingregister", or (in English - not quite verbatim) "The largest twin register in the world", accessed 28 October 2002. [Back] 121. See Cederlöf, R., "Statement to the Congressional Committee", 1968, Bates: 2015052918/2932. [Back] 122. William W. Shinn (of law firm Shook, Hardy, Ottman, Mitchell & Bacon) to Alex Holtzmann, 14 December 1967, Bates: 1005050082/0084. [Back] 123. News summary, The Tobacco Institute, 28 April 1969, Bates: 2015039344. Swedish daily Svenska Dagbladet wrote about the study on December 3 1973, "Svenska forskarrön: Personligheten mer dödande än rökningen", here in English translation, "Swedish Research Study: Personality Deadlier Than Smoking". [Back] 124. Letter from Ehud Hominer to Andrew Wist (PM Australia) 27 August 1969, Bates: 2015048054. [Back] 125. CTR, Council for Tobacco Research; S, D., "Lars Friberg, M.D., the Karolinska Institute, Stockholm New Application No. 1037 'cause of Death in Relation to Smoking Habits and Other Behavorial and Enviromental Factors. A Study on the Swedish Twin Registry'. Grant Application No. 1037", 26 June 1975, Bates: 1003540731/0733. [Back] 126. Lee C.Y., Glantz S.A., "The Tobacco Industry's Successful Efforts to Control Tobacco Policy Making in Switzerland", University of California, San Francisco, 2001, p. 30. [Back] 127. Letter from H. Wakeham to Alex Holtzman, 11 July 1973, Bates: 1000053116. [Back] 128. Letter to Don Hoel and Alex Holtzman from H Wakeham, 16 August 1974, Bates: 1004863825. [Back] 129. Letter to Richard Carchman, 23 June 1997, Bates: 2063590609. [Back] 130. "Inside the Tobacco Deal. Interviews: Dr. Gary Huber", Frontline Online, 12 May 1998. [Back] 131. Ross E., "WHO: Tobacco Even More Cancerous", Associated Press, 19 June, 2002. [Back] 132. "Tobacco Industry Statements in the Department of Justice Lawsuit", Prepared for Rep. Henry A. Waxman, Minority Staff Report, Special Investigations Division, Committee on Government Reform, U.S. House of Representatives, September 17, 2002. At this address you may also find the answers submitted by the tobacco companies, which constitute a lesson from the upper school of judicial acrobatics. [Back] 133. The BF Goodrich Company (till Union Carbide, Imperial Chemical Industries, och The Monsanto Company), "Summary of meeting Cincinnati, Ohio: Hand disease occuring during polymerisation of polyvinyl chloride", 6-7 June, 1966 (PDF). [Back]
134. Suciu I., Drejman I., Valaskai M., "Investigation of the diseases produced by vinyl chloride", Medicina interna (Bucharest) 15:967-78 (Aug.), 1963 (PDF). 135. Union Carbide Corporation, Plastics Division, South Charleston Plant, letter from R.N. Wheeler Jr, October 24, 1966 (PDF). [Back] 136. CMA Vinyl Chloride Technical Panel Meeting, March 4, 1980 (PDF). [Back] 137. CMA Vinyl Chloride Technical Panel Meeting, March 4, 1980 (PDF). [Back] 138. See "Grassroots: The Chemical Industry's Astroturf Agenda", accessed 16 December 2002. [Back] 139. Lowray W.C., "Report to the board", September 8, 1980, CMA documents 072735-072740, p. 4 (PDF). [Back] 140. "CMA Grassroots program 1984", CMA documents 074816-074823, p. 1 (PDF). [Back] 141. "Statement of the American Chemistry Council Regarding Findings of Applied Epidemiology, Inc. on Vinyl Chloride Monomer", 26 January 1999. [Back] 142. "The Source Newsletter", PPG Industries och Vista Chemical Company, Lake Charles, volym 1 no 3, 1995, [auth. Dan McGinn, PPG's Manager of Communications] (PDF). [Back] 143. Green S.J., "Smoking, Associated Diseases and Causality", 1 January 1980, p. 1, Brown & Williamson: 1192.02.[Back] 144. "The Roper Proposal", a confidential memo from Tobacco Institute's Fred Panzer to Tobacco Institute Assist. Vice-President of Public Relations Horace R Kornegay, May 1, 1972, Bates: 2024274199/4202. [Back] 145. The Janus-faced dioxin industry clearly showed its other side at, for instance, the case of Kemner et al. v. Monsanto Company, 1985, when it was revealed that one of the key studies often referred to by Monsanto as showing the harmlessness of dioxin, a study made by Judith Zack and Bill Gaffey, was in fact forged. The study gave the impression that several of the persons who died from cancer were not part of the group that had been exposed to dioxins, when in fact they were. In another study, by Raymond Suskind and V. S. Hertzberg, the method was reversed: here the dioxin exposure was accounted for, but the diseased cases were concealed. See Rachel's Environment & Health Weekly, no 494, and "Collected Papers of William Sanjour, The Monsanto Investigation", 20 July 1994. [Back] 146. Cedervall B. et al., "Forskargrupp kritiserar falsklarm om strålningsrisk: 'Mobiltelefonen ofarlig'" ["Scientist group criticizes false alerts about radiation hazards: 'Mobile phones are safe'"], Dagens Nyheter, 18 July 2002. Although the authors claim that it would be impossible to prove even that raspberry juice is not carcinogenic, they do not hesitate in ending their article with the conclusion that exposure to electromagnetic fields "does not constitute a risk for cancer or genetic injury."[Back] 147. Modell W., "Chairman's closing remarks", i Wolstenholme & Porter [red.], Drug Responses in Man, 1967. [Back] 148. Sjöström H., Nilsson R., Thalidomide and the power of the drug companies, 1972. p. 161. [Back] 149. Pepples E., "Cigarette Smoking And Health, What Are The Facts?", October 3, 1967, Brown & Williamson: 1903.02. [Back] 150. Green S., Cigarette Smoking and Causality (marked up draft, 19??), Brown & Williamson: 1192.01. [Back] 151. Åmark K., "Arbetets sjukdomar", Forskning och framsteg, no 8, 2000, p. 40. [Back] 152. Frey A.H.:, "Headaches from Cellular Telephones: Are They Real and What Are the Implications?", Environmental Health Perspectives, 106: 3, March 1998. [Back] 153. "Mystery in the skin: Screen dermatitis, the effect of computer work on human skin. An interview with associate professor Olle Johansson", FEB October 2001. [Back] 154. Carlsson A., "Aktuella problem rörande fluoriders farmakologi och toxikologi" ["Current problems concerning the pharmacology and toxicology of fluorides"], Läkartidningen, no 14, 1978. [Back] 155. Graham-Rowe D., "Cancer cell study revives cellphone safety fears", New Scientist, 24 October 2002. The study in question is Marinelli F., La Sala D., Cattini L., Tomassetti G., Zamparelli A., "900 MHz electromagnetic field affects gene expression in cultured T-lymphoblastic leukaemia cells", executed at Istituto di Citomorfologia, Consiglio Nazionale delle Ricerche, Bologna. The study was presented at the International Workshop on Biological Effects of Electromagnetic Fields, Greece, October 2002. [Back] 156. Johansson L:, "Wallström försvarar ny dioxingräns", Dagens Nyheter, 6 October 2001. [Back] 157. Landell N.E., "Miljödebatten har borrats i sank", Svenska Dagbladet, 31 July 2001. [Back] 158. Colborn T., Dumanoski D., Myers J.P., Our stolen future, 1996, kap. 11 "Beyond Cancer". [Back] 159. Hrobjartsson A., Gotzsche P.C., "Is the placebo powerless? An analysis of clinical trials comparing placebo with no treatment", N Engl J Med, 2001 May 24;344(21):1594-602 [Back] 160. Beecher H.K., "The powerful placebo", The Journal of the American Medical Association, 159, 1955, p. 1602-1606 [Back] 161. When this is being written, there are also trials going on where people who claim that they have been afflicted with cancer from mobile phone radiation, have sued the mobile phone industry for billions of dollars. See RCR Wireless News. [Back] 162. See for instance ToxicTeeth.net. On November 14, 2002 a hearing was held in the US House of Representatives about the state of research regarding dental amalgam, an initiative by rep. Dan Burton with statements by i.a. Dr. Boyd Haley. [Back] 163. Smith R., "Maintaining the integrity of the scientific record", The British Medical Journal, 15 September, 2001;323:588. See also the International Committee of Medical Journal Editors. [Back] 164. Okie S., "A Stand for Scientific Independence: Medical Journals Aim to Curtail Drug Companies' Influence", The Washington Post, 5 August 2001 [Back] 165. Monbiot G., "The fake persuaders: Corporations are inventing people to rubbish their opponents on the internet", The Guardian, 14 May 2002. Bivings later denied these allegations in Gary Bivings, "Bivings: we condemn online vandalism", The Guardian, 12 June 2002. [Back] 166. Bronowski J., Science and human values, 1956, [1965], p. 6. [Back] 167. Latour B., Woolgar S., Laboratory life: The construction of scientific facts, 2 ed., 1986 p. 46. [Back]
Copyright © Karl-Erik Tallmo, 2003.
| ||||||||||||||||||||||
About the author
Links to sections:
All issues | Articles and essays | Origo | The Gallery | Contributors
[English Homepage] | [Svensk bassida]